

Timing of Recanalization and Functional Recovery in Acute Ischemic Stroke
- PMID: 32027798
- PMCID: PMC7005347
- DOI: 10.5853/jos.2019.01648
Timing of Recanalization and Functional Recovery in Acute Ischemic Stroke
Abstract
Background and purpose: Although onset-to-treatment time is associated with early clinical recovery in acute ischemic stroke (AIS) patients treated with intravenous tissue plasminogen activator (tPA), the effect of the timing of tPA-induced recanalization on functional outcomes remains debatable.
Methods: We conducted a multicenter, prospective observational cohort study to determine whether early (within 1-hour from tPA-bolus) complete or partial recanalization assessed during 2-hour real-time transcranial Doppler monitoring is associated with improved outcomes in patients with proximal occlusions. Outcome events included dramatic clinical recovery (DCR) within 2 and 24-hours from tPA-bolus, 3-month mortality, favorable functional outcome (FFO) and functional independence (FI) defined as modified Rankin Scale (mRS) scores of 0-1 and 0-2 respectively.
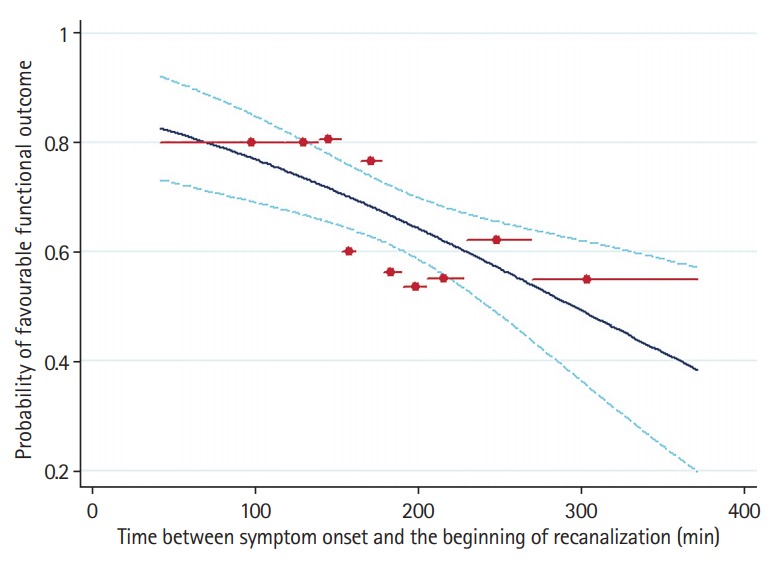
Results: We enrolled 480 AIS patients (mean age 66±15 years, 60% men, baseline National Institutes of Health Stroke Scale score 15). Patients with early recanalization (53%) had significantly (P<0.001) higher rates of DCR at 2-hour (54% vs. 10%) and 24-hour (63% vs. 22%), 3-month FFO (67% vs. 28%) and FI (81% vs. 39%). Three-month mortality rates (6% vs. 17%) and distribution of 3-month mRS scores were significantly lower in the early recanalization group. After adjusting for potential confounders, early recanalization was independently associated with higher odds of 3-month FFO (odds ratio [OR], 6.19; 95% confidence interval [CI], 3.88 to 9.88) and lower likelihood of 3-month mortality (OR, 0.34; 95% CI, 0.17 to 0.67). Onset to treatment time correlated to the elapsed time between tPA-bolus and recanalization (unstandardized linear regression coefficient, 0.13; 95% CI, 0.06 to 0.19).
Conclusions: Earlier tPA treatment after stroke onset is associated with faster tPA-induced recanalization. Earlier onset-to-recanalization time.
Results: in improved functional recovery and survival in AIS patients with proximal intracranial occlusions.
Keywords: Outcomes; Reperfusion; Stroke; Thrombolysis.
Figures

References
-
- Hacke W, Donnan G, Fieschi C, Kaste M, von Kummer R, Broderick JP, et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet. 2004;363:768–774. - PubMed
-
- Emberson J, Lees KR, Lyden P, Blackwell L, Albers G, Bluhmki E, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet. 2014;384:1929–1935. - PMC - PubMed
-
- Tsivgoulis G, Katsanos AH, Kadlecová P, Czlonkowska A, Kobayashi A, Brozman M, et al. Intravenous thrombolysis for ischemic stroke in the golden hour: propensity-matched analysis from the SITS-EAST registry. J Neurol. 2017;264:912–920. - PubMed
-
- Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke. 2007;38:967–973. - PubMed
-
- Tsivgoulis G, Alexandrov AV. Does “time is brain” also mean “time is clot”? Time dependency of tissue-type plasminogen activator-induced recanalization in acute ischemic stroke. Stroke. 2014;45:2555–2556. - PubMed
