

Classification of Current Procedural Terminology Codes from Electronic Health Record Data Using Machine Learning
- PMID: 32028374
- PMCID: PMC7665375
- DOI: 10.1097/ALN.0000000000003150
Classification of Current Procedural Terminology Codes from Electronic Health Record Data Using Machine Learning
Abstract
Background: Accurate anesthesiology procedure code data are essential to quality improvement, research, and reimbursement tasks within anesthesiology practices. Advanced data science techniques, including machine learning and natural language processing, offer opportunities to develop classification tools for Current Procedural Terminology codes across anesthesia procedures.
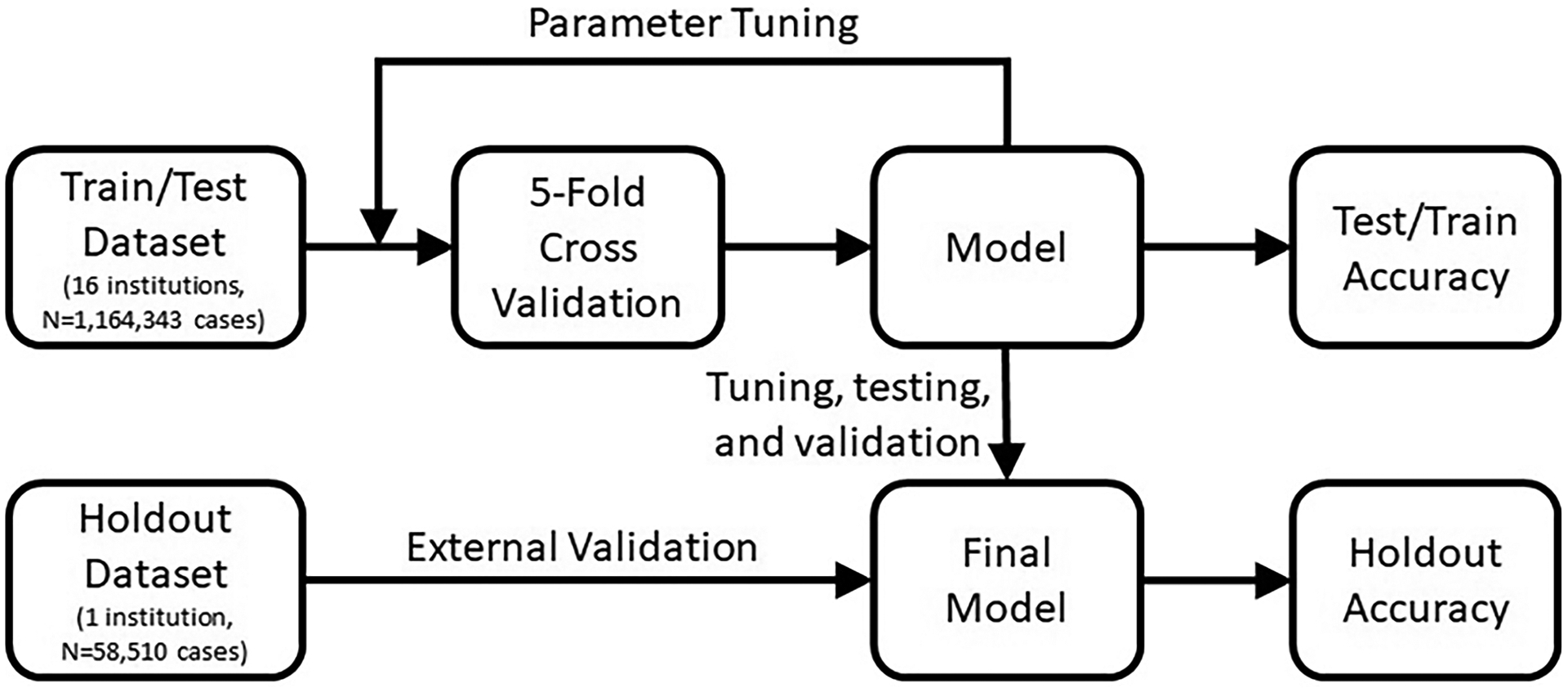
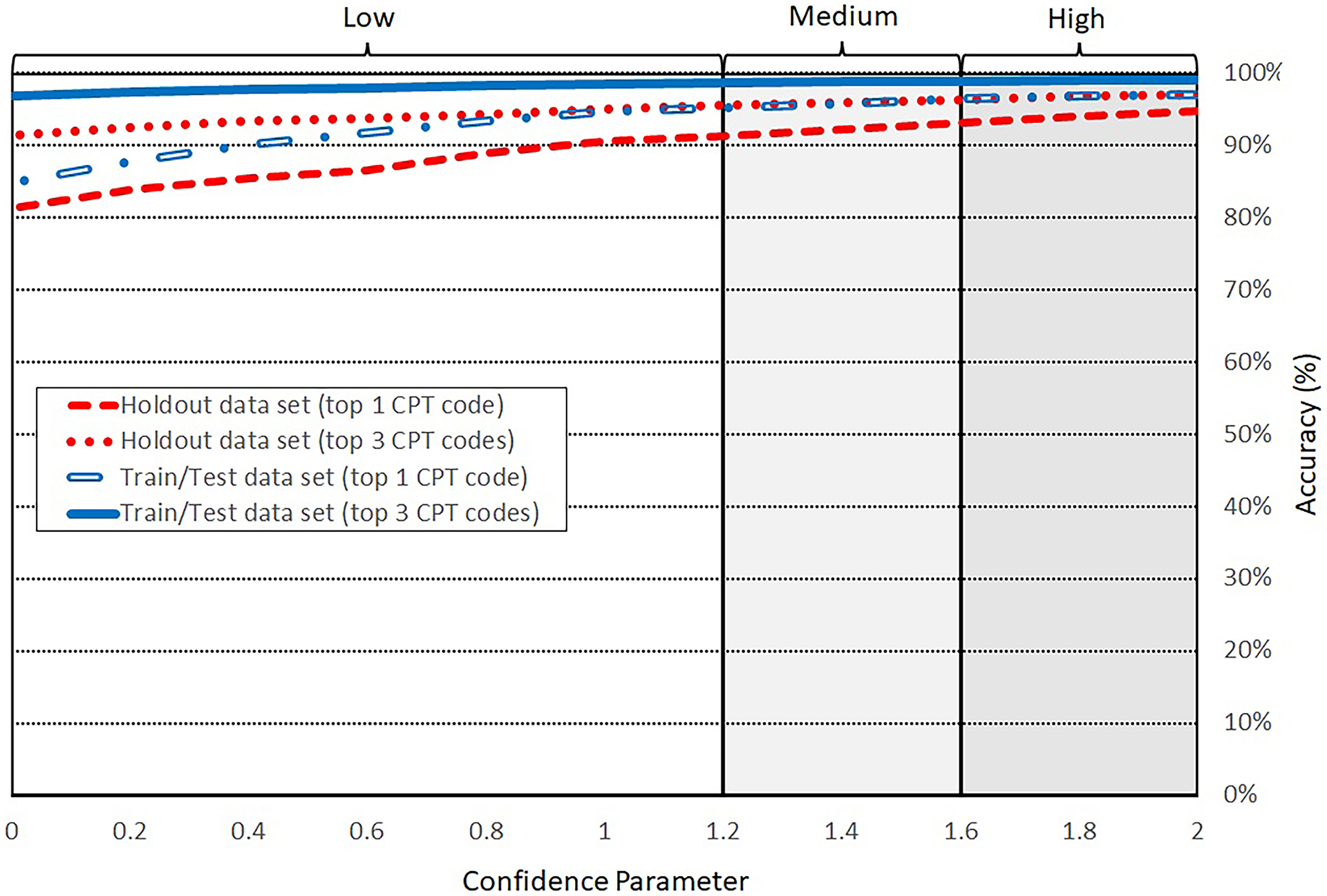
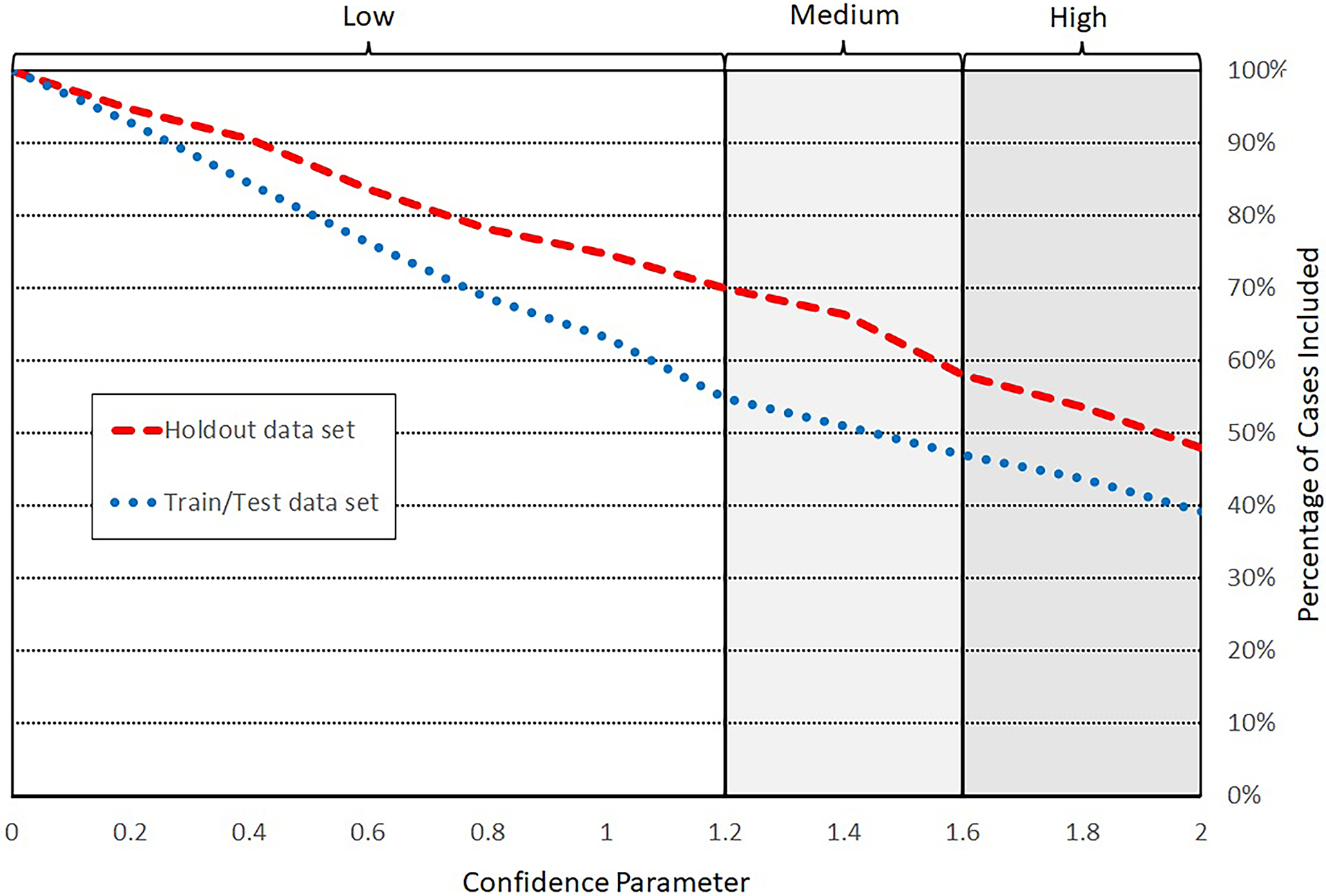
Methods: Models were created using a Train/Test dataset including 1,164,343 procedures from 16 academic and private hospitals. Five supervised machine learning models were created to classify anesthesiology Current Procedural Terminology codes, with accuracy defined as first choice classification matching the institutional-assigned code existing in the perioperative database. The two best performing models were further refined and tested on a Holdout dataset from a single institution distinct from Train/Test. A tunable confidence parameter was created to identify cases for which models were highly accurate, with the goal of at least 95% accuracy, above the reported 2018 Centers for Medicare and Medicaid Services (Baltimore, Maryland) fee-for-service accuracy. Actual submitted claim data from billing specialists were used as a reference standard.
Results: Support vector machine and neural network label-embedding attentive models were the best performing models, respectively, demonstrating overall accuracies of 87.9% and 84.2% (single best code), and 96.8% and 94.0% (within top three). Classification accuracy was 96.4% in 47.0% of cases using support vector machine and 94.4% in 62.2% of cases using label-embedding attentive model within the Train/Test dataset. In the Holdout dataset, respective classification accuracies were 93.1% in 58.0% of cases and 95.0% among 62.0%. The most important feature in model training was procedure text.
Conclusions: Through application of machine learning and natural language processing techniques, highly accurate real-time models were created for anesthesiology Current Procedural Terminology code classification. The increased processing speed and a priori targeted accuracy of this classification approach may provide performance optimization and cost reduction for quality improvement, research, and reimbursement tasks reliant on anesthesiology procedure codes.
Conflict of interest statement
Conflicts of Interest:
This work has been declared through the University of Michigan Office of Tech Transfer and a provisional patent (U.S. Provisional Application No.: 62/791,257) has been filed related to the work presented in this study.
Figures
References
-
- 2018 CROSSWALK Book: A Guide for Surgery/Anesthesia CPT Codes. American Society of Anesthesiologists; 2017.
-
- CPT 2018, Current procedural terminology 2018: Professional edition. American Medical Association; 2017.
-
- Polsky D, Candon M, Saloner B, et al. Changes in primary care access between 2012 and 2016 for new patients with medicaid and private coverage. JAMA Internal Medicine. 2017;177(4):588–590. - PubMed
-
- Holt J, Warsy A, Wright P. Medical decision making: guide to improved CPT coding. South Med J. 2010;103(4):316–322. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
