

Association Between Time of Day and the Decision for an Intrapartum Cesarean Delivery
- PMID: 32028489
- PMCID: PMC7595762
- DOI: 10.1097/AOG.0000000000003707
Association Between Time of Day and the Decision for an Intrapartum Cesarean Delivery
Abstract
Objective: To examine whether the decision and indications for performing intrapartum cesarean delivery vary by time of day.
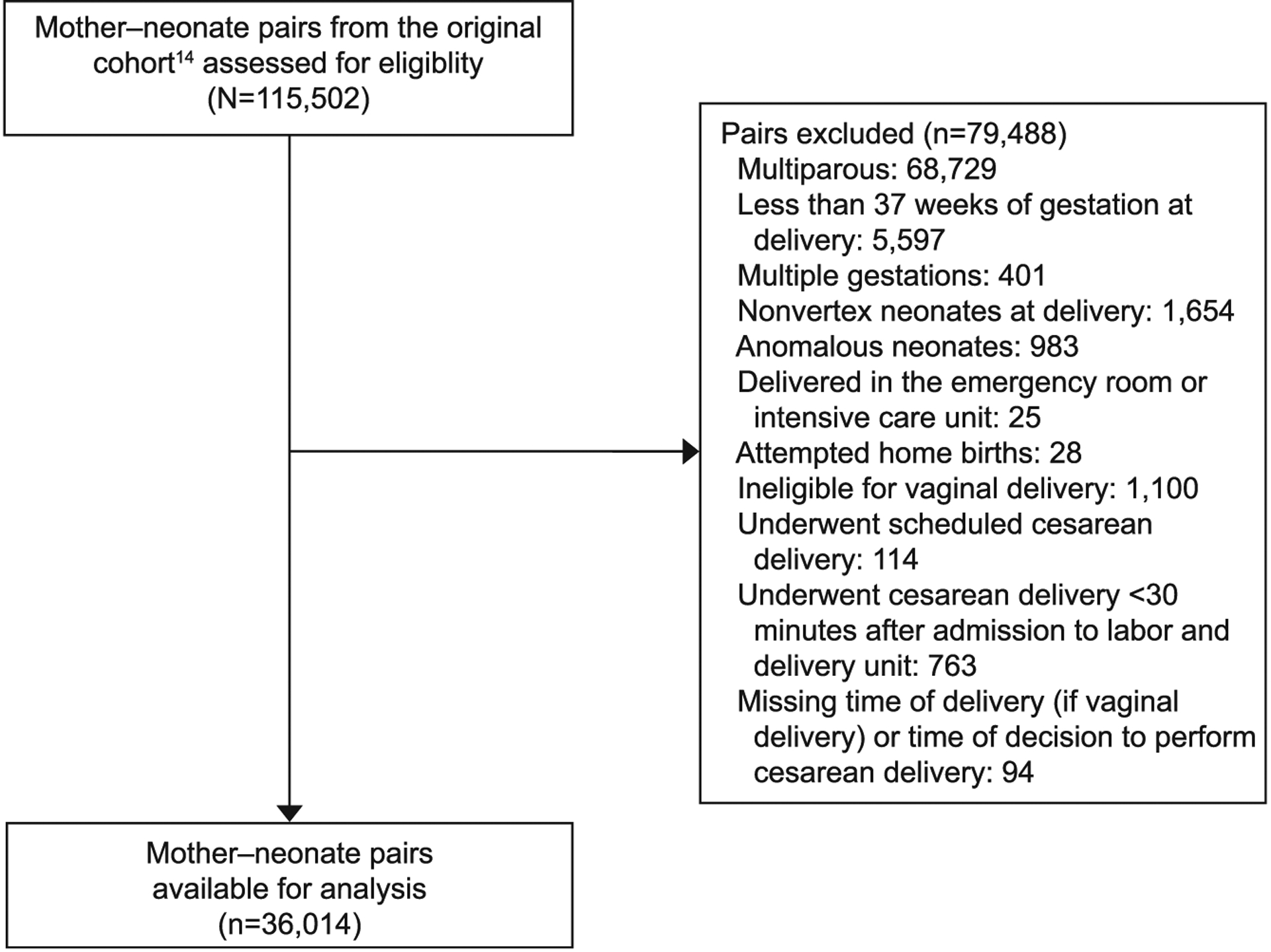
Methods: We conducted a secondary analysis of a multicenter observational cohort of 115,502 deliveries (2008-2011), including nulliparous women with term, singleton, nonanomalous live gestations in vertex presentation who were attempting labor. Those who attempted home birth, or underwent cesarean delivery scheduled or decided less than 30 minutes after admission were excluded. Time of day was defined as cesarean delivery decision time among those who delivered by cesarean and delivery time among those who delivered vaginally, categorized by each hour of a 24-hour day. Primary outcomes were decision to perform cesarean delivery and the indications for cesarean delivery (labor dystocia, nonreassuring fetal status, or other indications). Secondary outcomes included whether a dystocia indication adhered to standards promoted to reduce cesarean delivery rates. Bivariate analyses were performed using χ and Kruskal-Wallis tests for categorical and continuous outcomes, respectively, and generalized additive models with smoothing splines explored nonlinear associations without adjustment for other factors.
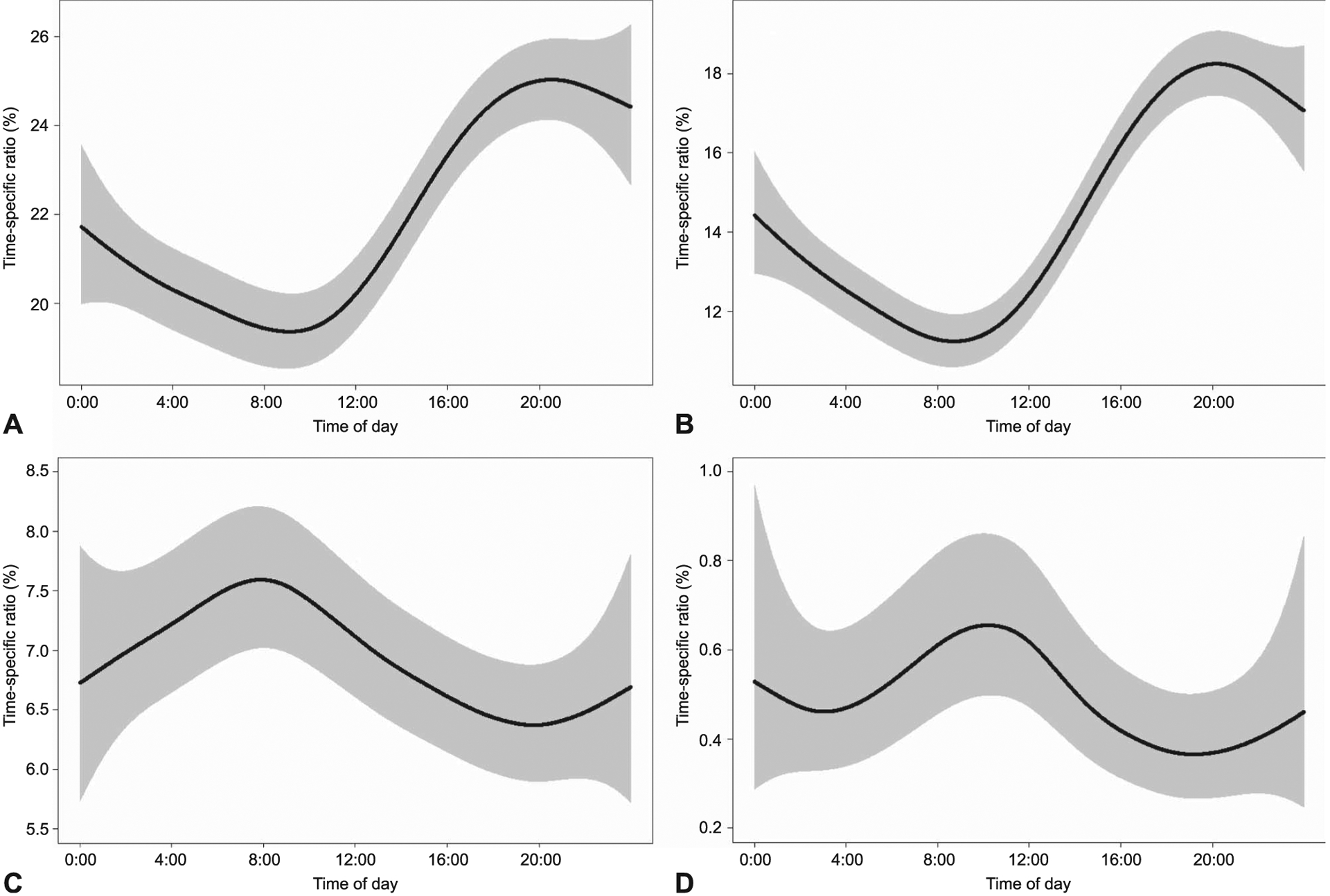
Results: Seven thousand nine hundred fifty-six (22.1%) of 36,014 eligible women underwent cesarean delivery. Decision for cesarean delivery (P<.001) decreased from midnight (21.2%) to morning, reaching a nadir at 10:00 (17.9%) and subsequently rising to peak at 21:00 (26.2%). The frequency of cesarean delivery for dystocia also was significantly associated with time of day (P<.001) in a pattern mirroring overall cesarean delivery. Among cesarean deliveries for dystocia (n=5,274), decision for cesarean delivery at less than 5 cm dilation (P<.001), median duration from 5 cm dilation to cesarean delivery decision (P=.003), and median duration from complete dilation to cesarean delivery decision (P=.014) all significantly differed with time of day. The frequency of nonreassuring fetal status and "other" indications were not significantly associated with time of day (P>.05).
Conclusion: Among nulliparous women who were attempting labor at term, the decision to perform cesarean delivery, particularly for dystocia, varied with time of day. Some of these differences correlate with labor management differences, given the changing frequency of latent phase cesarean delivery and median time in active phase.
Figures
References
-
- Martin JA, Hamilton BE, Osterman MJ, Driscoll AK, Mathews TJ. Births: final data for 2015. Natl Vital Stat Rep 2017;66:1. - PubMed
-
- Osterman MJ, Martin JA. Trends in low-risk cesarean delivery in the United States, 1990–2013. Natl Vital Stat Rep 2014;63: 1–16. - PubMed
-
- Rhodes JC, Schoendorf KC, Parker JD. Contribution of excess weight gain during pregnancy and macrosomia to the cesarean delivery rate. Pediatrics 2003;111(5 pt 2):1181–5. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD040500/HD/NICHD NIH HHS/United States
- UG1 HD027869/HD/NICHD NIH HHS/United States
- UG1 HD040560/HD/NICHD NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- UG1 HD053097/HD/NICHD NIH HHS/United States
- UG1 HD027915/HD/NICHD NIH HHS/United States
- U10 HD040485/HD/NICHD NIH HHS/United States
- U10 HD034116/HD/NICHD NIH HHS/United States
- U10 HD027869/HD/NICHD NIH HHS/United States
- U10 HD027917/HD/NICHD NIH HHS/United States
- UG1 HD040485/HD/NICHD NIH HHS/United States
- U10 HD040560/HD/NICHD NIH HHS/United States
- UG1 HD040500/HD/NICHD NIH HHS/United States
- U10 HD040512/HD/NICHD NIH HHS/United States
- U10 HD040545/HD/NICHD NIH HHS/United States
- U01 HD036801/HD/NICHD NIH HHS/United States
- U10 HD053118/HD/NICHD NIH HHS/United States
- UL1 RR024989/RR/NCRR NIH HHS/United States
- U10 HD040544/HD/NICHD NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- UL1 RR025764/RR/NCRR NIH HHS/United States
- UG1 HD034116/HD/NICHD NIH HHS/United States
- UG1 HD040544/HD/NICHD NIH HHS/United States
- UG1 HD034208/HD/NICHD NIH HHS/United States
- UG1 HD040512/HD/NICHD NIH HHS/United States
- U10 HD027915/HD/NICHD NIH HHS/United States
- UG1 HD040545/HD/NICHD NIH HHS/United States
- U10 HD034208/HD/NICHD NIH HHS/United States
- U10 HD053097/HD/NICHD NIH HHS/United States
- P2C HD050924/HD/NICHD NIH HHS/United States
- U10 HD021410/HD/NICHD NIH HHS/United States
- U10 HD036801/HD/NICHD NIH HHS/United States
- U24 HD036801/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
