

Use of Uterine Tamponade and Interventional Radiology Procedures During Delivery Hospitalizations
- PMID: 32028498
- PMCID: PMC7040521
- DOI: 10.1097/AOG.0000000000003722
Use of Uterine Tamponade and Interventional Radiology Procedures During Delivery Hospitalizations
Abstract
Objective: To characterize use of uterine tamponade and interventional radiology procedures.
Methods: This retrospective study analyzed uterine tamponade and interventional radiology procedures in a large administrative database. The primary outcomes were temporal trends in these procedures 1) during deliveries, 2) by hospital volume, and 3) before hysterectomy for uterine atony or delayed postpartum hemorrhage. Three 3-year periods were analyzed: 2006-2008, 2009-2011, and 2012-2014. Risk of morbidity in the setting of hysterectomy with uterine tamponade and interventional radiology procedures as the primary exposures was additionally analyzed in adjusted models.
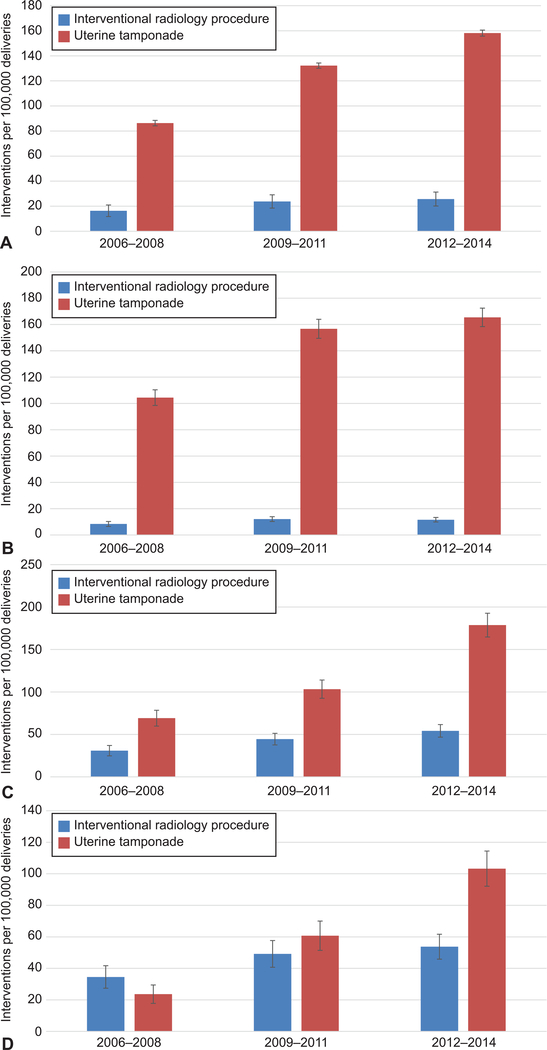
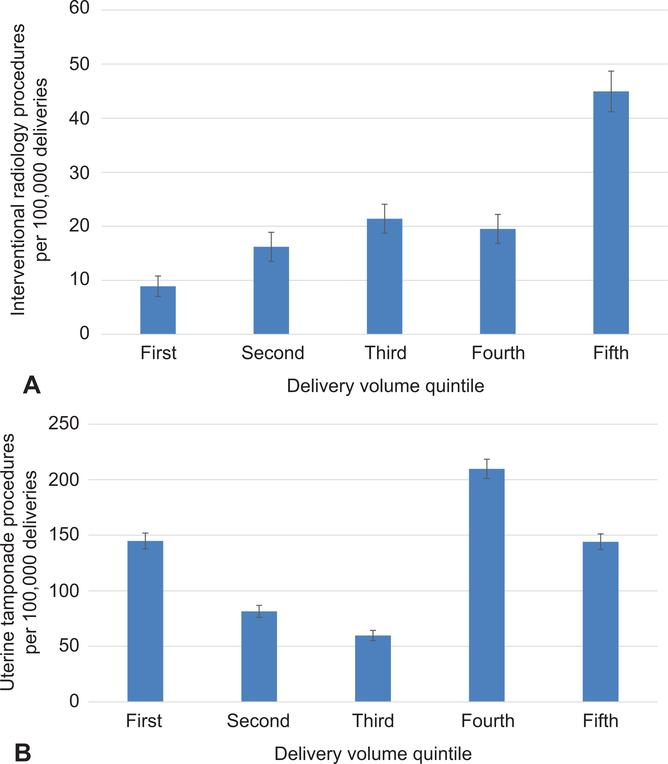
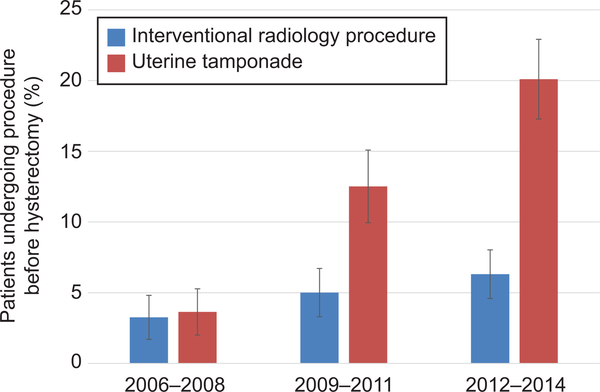
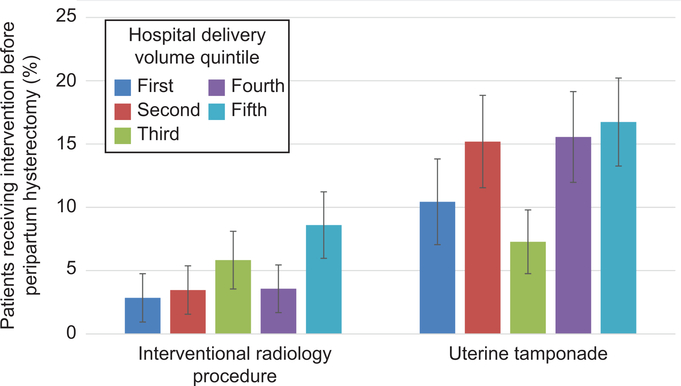
Results: The study included 5,383,486 deliveries, which involved 6,675 uterine tamponade procedures, 1,199 interventional radiology procedures, and 1,937 hysterectomies. Interventional radiology procedures increased from 16.4 to 25.7 per 100,000 delivery hospitalizations from 2006-2008 to 2012-2014 (P<.01), and uterine tamponade increased from 86.3 to 158.1 (P<.01). Interventional radiology procedures use was highest (45.0/100,000 deliveries, 95% CI 41.0-48.9) in the highest and lowest (8.9/100,000, 95% CI 7.1-10.7) in the lowest volume quintile. Uterine tamponade procedures were most common in the fourth (209.8/100,000, 95% CI 201.1-218.5) and lowest in the third quintile (59.8/100,000, 95% CI 55.1-64.4). Interventional radiology procedures occurred before 3.3% of hysterectomies from 2006 to 2008 compared with 6.3% from 2012 to 2014 (P<.05), and uterine tamponade procedures increased from 3.6% to 20.1% (P<.01). Adjusted risks for morbidity in the setting of uterine tamponade and interventional radiology before hysterectomy were significantly higher (adjusted risk ratio [aRR] 1.63, 95% CI 1.47-1.81 and aRR 1.75 95% CI 1.51-2.03, respectively) compared with when these procedures were not performed.
Conclusion: This analysis found that uterine tamponade and interventional radiology procedures became increasingly common over the study period, are used across obstetric volume settings, and in the setting of hysterectomy may be associated with increased risk of morbidity, although this relationship is not necessarily causal.
Conflict of interest statement
Figures
Similar articles
-
The impact of Bakri balloon tamponade on the rate of postpartum hysterectomy for uterine atony.J Matern Fetal Neonatal Med. 2017 May;30(10):1163-1166. doi: 10.1080/14767058.2016.1208742. Epub 2016 Jul 29. J Matern Fetal Neonatal Med. 2017. PMID: 27364858
-
Impact of uterine balloon tamponade on the use of invasive procedures in severe postpartum hemorrhage.Acta Obstet Gynecol Scand. 2017 Jul;96(7):877-882. doi: 10.1111/aogs.13130. Epub 2017 Apr 12. Acta Obstet Gynecol Scand. 2017. PMID: 28295136
-
Uterine balloon tamponade for the treatment of postpartum hemorrhage: a systematic review and meta-analysis.Am J Obstet Gynecol. 2020 Apr;222(4):293.e1-293.e52. doi: 10.1016/j.ajog.2019.11.1287. Epub 2020 Jan 6. Am J Obstet Gynecol. 2020. PMID: 31917139
-
Comparison of outcome between intrauterine balloon tamponade and uterine artery embolization in the management of persistent postpartum hemorrhage: A propensity score-matched cohort study.Acta Obstet Gynecol Scand. 2019 Nov;98(11):1473-1482. doi: 10.1111/aogs.13679. Epub 2019 Jul 10. Acta Obstet Gynecol Scand. 2019. PMID: 31240693
-
Impact of intrauterine balloon tamponade on emergency peripartum hysterectomy following vaginal delivery.Eur J Obstet Gynecol Reprod Biol. 2021 Jan;256:125-129. doi: 10.1016/j.ejogrb.2020.10.064. Epub 2020 Nov 2. Eur J Obstet Gynecol Reprod Biol. 2021. PMID: 33207298 Review.
Cited by
-
What we talk about when we talk about severe maternal morbidity: a call to action to critically review severe maternal morbidity as an outcome measure.Am J Obstet Gynecol MFM. 2023 May;5(5):100882. doi: 10.1016/j.ajogmf.2023.100882. Epub 2023 Feb 1. Am J Obstet Gynecol MFM. 2023. PMID: 36736823 Free PMC article.
References
-
- Berg CJ, Harper MA, Atkinson SM, Bell EA, Hage ML. Preventability of pregnancy-related deaths - results of a state-wide review. Obstet Gynecol 2005;206:1228–34. - PubMed
-
- Main EK. Decisions required for operating a maternal mortality review committee: the California experience. Semin Perinatol 2012;36:37–41. - PubMed
-
- Main E, Goffman D, Scavone B, et al. National Partnership for Maternal Safety Consensus Bundle on Obstetric Hemorrhage. Obstet Gynecol 2015;126:155–62. - PubMed
-
- Kramer MS, Berg C, Abenhaim H, et al. Incidence, risk factors, and temporal trends in severe postpartum hemorrhage. Am J Obstet Gynecol 2013;209:449 e1–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
