Angiotensin I and angiotensin II concentrations and their ratio in catecholamine-resistant vasodilatory shock
- PMID: 32028998
- PMCID: PMC7006163
- DOI: 10.1186/s13054-020-2733-x
Angiotensin I and angiotensin II concentrations and their ratio in catecholamine-resistant vasodilatory shock
Abstract
Background: In patients with vasodilatory shock, plasma concentrations of angiotensin I (ANG I) and II (ANG II) and their ratio may reflect differences in the response to severe vasodilation, provide novel insights into its biology, and predict clinical outcomes. The objective of these protocol prespecified and subsequent post hoc analyses was to assess the epidemiology and outcome associations of plasma ANG I and ANG II levels and their ratio in patients with catecholamine-resistant vasodilatory shock (CRVS) enrolled in the Angiotensin II for the Treatment of High-Output Shock (ATHOS-3) study.
Methods: We measured ANG I and ANG II levels at baseline, calculated their ratio, and compared these results to values from healthy volunteers (controls). We dichotomized patients according to the median ANG I/II ratio (1.63) and compared demographics, clinical characteristics, and clinical outcomes. We constructed a Cox proportional hazards model to test the independent association of ANG I, ANG II, and their ratio with clinical outcomes.
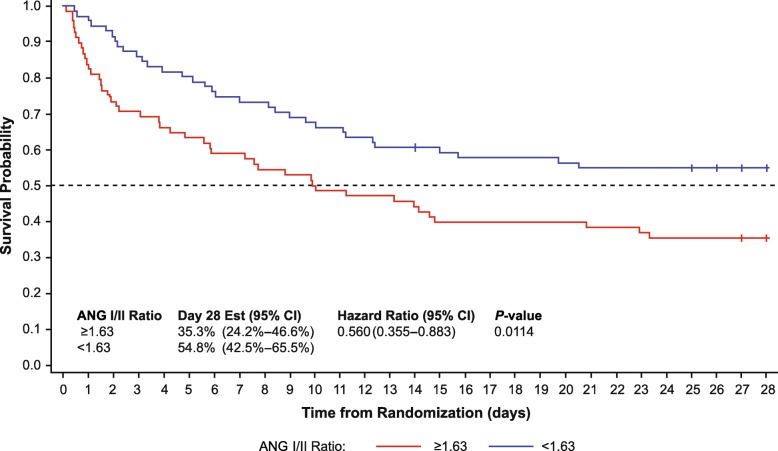
Results: Median baseline ANG I level (253 pg/mL [interquartile range (IQR) 72.30-676.00 pg/mL] vs 42 pg/mL [IQR 30.46-87.34 pg/mL] in controls; P < 0.0001) and median ANG I/II ratio (1.63 [IQR 0.98-5.25] vs 0.4 [IQR 0.28-0.64] in controls; P < 0.0001) were elevated, whereas median ANG II levels were similar (84 pg/mL [IQR 23.85-299.50 pg/mL] vs 97 pg/mL [IQR 35.27-181.01 pg/mL] in controls; P = 0.9895). At baseline, patients with a ratio above the median (≥1.63) had higher ANG I levels (P < 0.0001), lower ANG II levels (P < 0.0001), higher albumin concentrations (P = 0.007), and greater incidence of recent (within 1 week) exposure to angiotensin-converting enzyme inhibitors (P < 0.00001), and they received a higher norepinephrine-equivalent dose (P = 0.003). In the placebo group, a baseline ANG I/II ratio <1.63 was associated with improved survival (hazard ratio 0.56; 95% confidence interval 0.36-0.88; P = 0.01) on unadjusted analyses.
Conclusions: Patients with CRVS have elevated ANG I levels and ANG I/II ratios compared with healthy controls. In such patients, a high ANG I/II ratio is associated with greater norepinephrine requirements and is an independent predictor of mortality, thus providing a biological rationale for interventions aimed at its correction.
Trial registration: ClinicalTrials.gov identifier NCT02338843. Registered 14 January 2015.
Keywords: ACE; ACE dysfunction; Angiotensin I; Angiotensin II; Sepsis; Vasodilatory shock.
Conflict of interest statement
Rinaldo Bellomo, Richard G. Wunderink, Ashish K. Khanna, Marlies Ostermann, and Paul J. Young have nothing to disclose.
Harold Szerlip received personal fees from La Jolla Pharmaceutical Company during the conduct of the study.
Shane W. English’s research center (Ottawa Hospital Research Institute) received per-patient reimbursement from La Jolla Pharmaceutical company for research coordinator time.
Laurence W. Busse has received consulting fees from La Jolla Pharmaceutical Company.
Adam M. Deane’s employer at the time of study (Royal Adelaide Hospital) received per-patient reimbursement to the institution from La Jolla Pharmaceutical Company for research coordinator time.
Michael T. McCurdy has served on the speakers’ bureau for La Jolla Pharmaceutical Company.
Damian R. Handisides and Lakhmir S. Chawla are employees of La Jolla Pharmaceutical Company and own stock.
George F. Tidmarsh was an employee of La Jolla Pharmaceutical Company at the time of the analysis and owns stock.
Timothy E. Albertson received institutional research funding during the conduct of the study and speaking honoraria after the conduct of the study from La Jolla Pharmaceutical Company.
Figures