

Is haemoglobin below 7.0 g/dL an optimal trigger for allogenic red blood cell transfusion in patients admitted to intensive care units? A meta-analysis and systematic review
- PMID: 32029484
- PMCID: PMC7045194
- DOI: 10.1136/bmjopen-2019-030854
Is haemoglobin below 7.0 g/dL an optimal trigger for allogenic red blood cell transfusion in patients admitted to intensive care units? A meta-analysis and systematic review
Abstract
Objectives: We employed a comprehensive systematic review and meta-analysis to assess benefits and risks of a threshold of haemoglobin level below 7 g/dL versus liberal transfusion strategy among critically ill patients, and even patients with septic shock.
Design: Systematic review and meta-analysis.
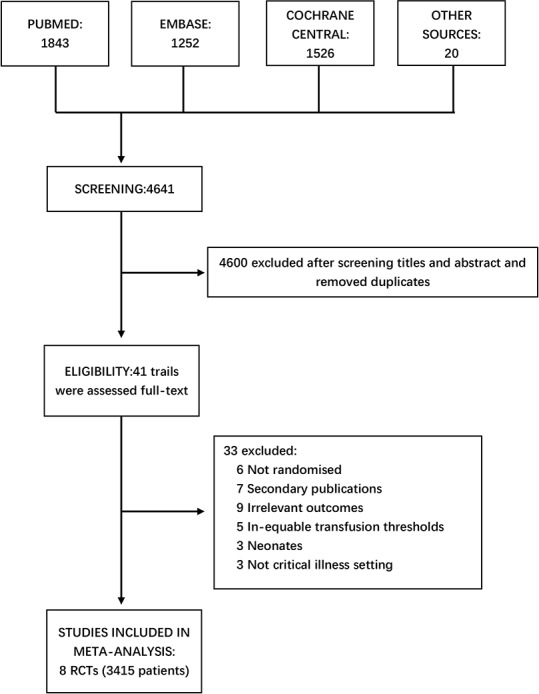
Data sources: We performed systematical searches for relevant randomised controlled trials (RCTs) in the Cochrane Library, EMBASE and PubMed databases up to 1 September 2019.
Eligibility criteria: RCTs among adult intensive care unit (ICU) patients comparing 7 g/dL as restrictive strategy with liberal transfusion were incorporated.
Data extraction and synthesis: The clinical outcomes, including short-term mortality, length of hospital stay, length of ICU stay, myocardial infarction (MI) and ischaemic events, were screened and analysed after data collection. We applied odds ratios (ORs) to analyse dichotomous outcomes and standardised mean differences (SMDs) to analyse continuous outcomes with fixed or random effects models based on heterogeneity evaluation for each outcome.
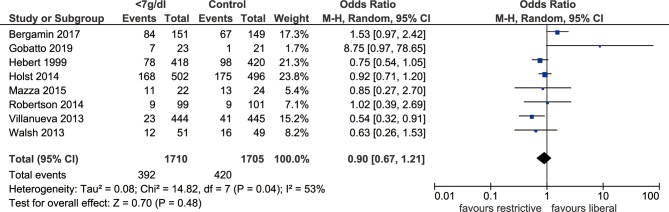
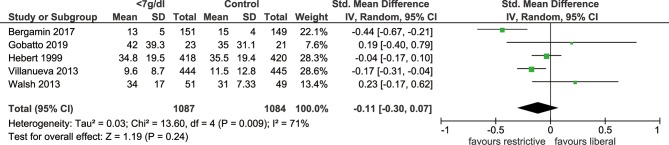
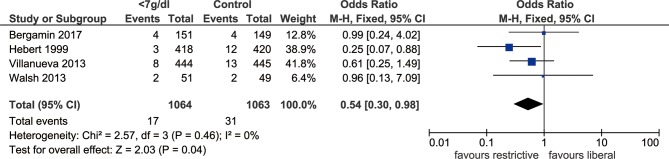
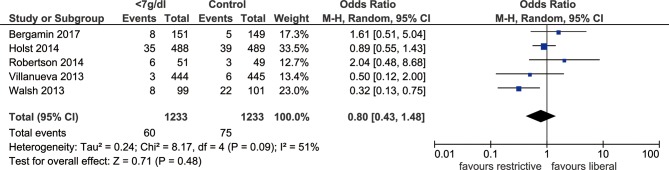
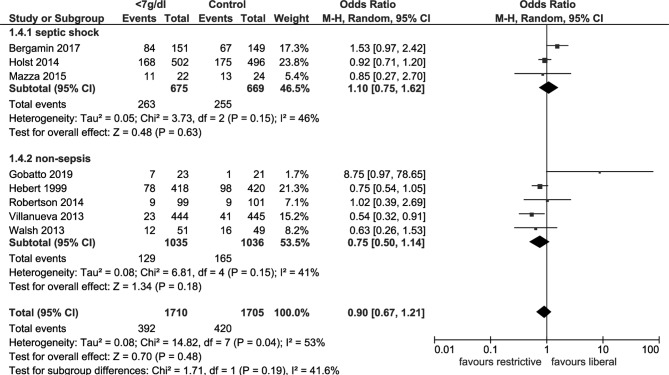
Results: Eight RCTs with 3415 patients were included. Compared with a more liberal threshold, a red blood cell (RBC) transfusion threshold <7 g/dL haemoglobin showed no significant difference in short-term mortality (OR: 0.90, 95% CI: 0.67 to 1.21, p=0.48, I2=53%), length of hospital stay (SMD: -0.11, 95% CI: -0.30 to 0.07, p=0.24, I2=71%), length of ICU stay (SMD: -0.03, 95% CI: -0.14 to 0.08, p=0.54, I2=0%) or ischaemic events (OR: 0.80, 95% CI: 0.43 to 1.48, p=0.48, I2=51%). However, we found that the incidence of MI (OR: 0.54, 95% CI: 0.30 to 0.98, p=0.04, I2=0%) was lower in the group with the threshold <7 g/dL than that with the more liberal threshold.
Conclusions: An RBC transfusion threshold <7 g/dL haemoglobin is incapable of decreasing short-term mortality in ICU patients according to currently published evidences, while it might have potential role in reducing MI incidence.
Keywords: intensive care units; red blood cells; septic shock; transfusion.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical