

Pan-Cancer Efficacy of Vemurafenib in BRAF V600-Mutant Non-Melanoma Cancers
- PMID: 32029534
- PMCID: PMC7196502
- DOI: 10.1158/2159-8290.CD-19-1265
Pan-Cancer Efficacy of Vemurafenib in BRAF V600-Mutant Non-Melanoma Cancers
Abstract
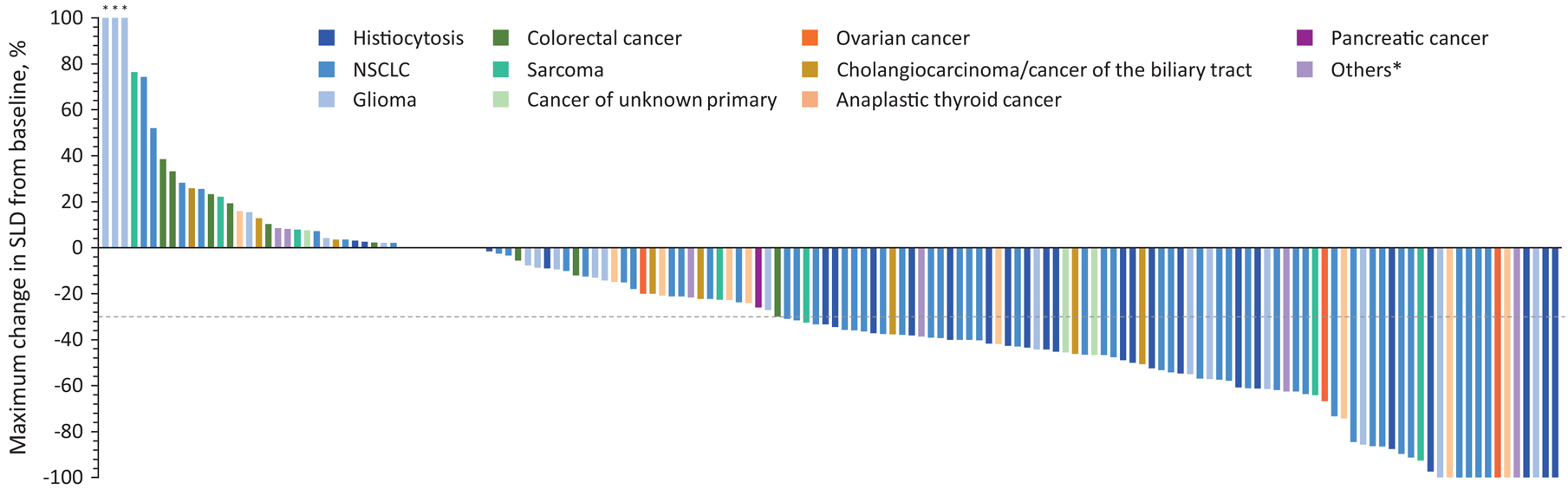
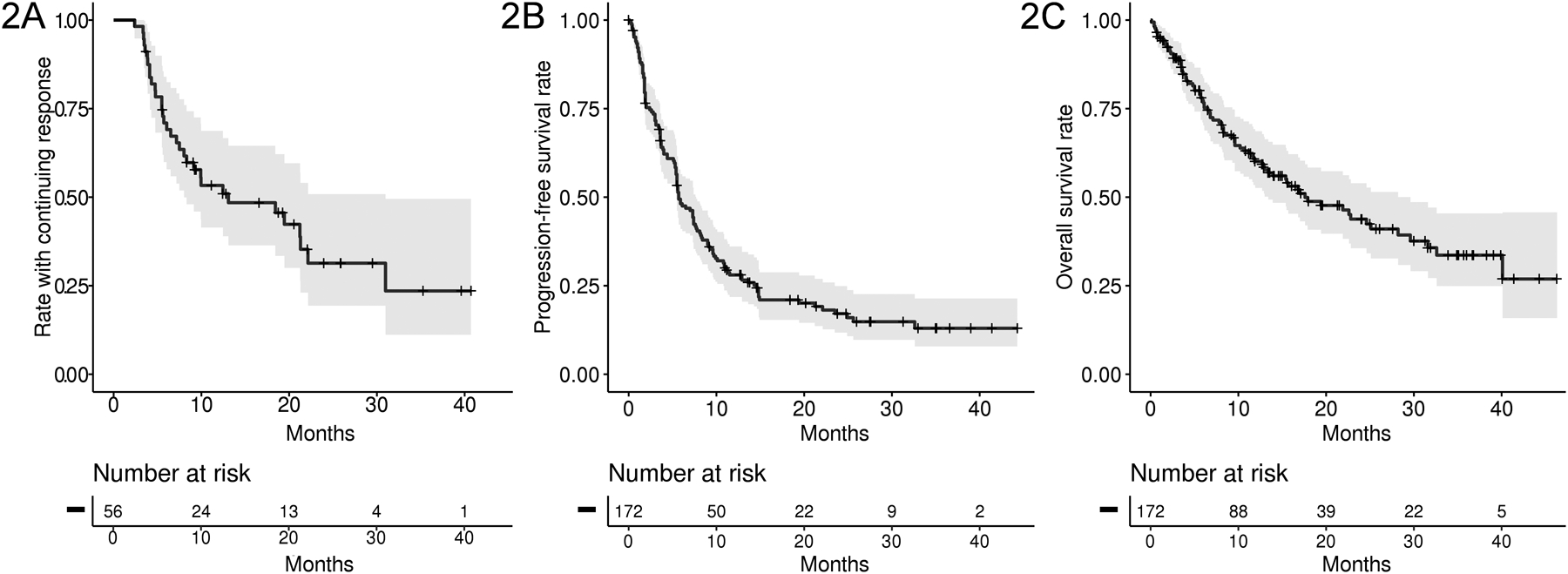
BRAF V600 mutations occur in a wide range of tumor types, and RAF inhibition has become standard in several of these cancers. Despite this progress, BRAF V600 mutations have historically been considered a clear demonstration of tumor lineage context-dependent oncogene addiction, based predominantly on the insensitivity to RAF inhibition in colorectal cancer. However, the true broader activity of RAF inhibition pan-cancer remains incompletely understood. To address this, we conducted a multicohort "basket" study of the BRAF inhibitor vemurafenib in non-melanoma BRAF V600 mutation-positive solid tumors. In total, 172 patients with 26 unique cancer types were treated, achieving an overall response rate of 33% and median duration of response of 13 months. Responses were observed in 13 unique cancer types, including historically treatment-refractory tumor types such as cholangiocarcinoma, sarcoma, glioma, neuroendocrine carcinoma, and salivary gland carcinomas. Collectively, these data demonstrate that single-agent BRAF inhibition has broader clinical activity than previously recognized. SIGNIFICANCE: These data suggest that BRAF V600 mutations lead to oncogene addiction and are clinically actionable in a broad range of non-melanoma cancers, including tumor types in which RAF inhibition is not currently considered standard of care.See related commentary by Ribas and Lo, p. 640.This article is highlighted in the In This Issue feature, p. 627.
©2020 American Association for Cancer Research.
Figures

Comment in
-
Trying for a BRAF Slam Dunk.Cancer Discov. 2020 May;10(5):640-642. doi: 10.1158/2159-8290.CD-20-0231. Cancer Discov. 2020. PMID: 32357967 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
