

Spiral wire localization of lung nodules: procedure effectiveness and oncological usefulness
- PMID: 32030241
- PMCID: PMC6987988
- DOI: 10.21037/jtd.2019.11.74
Spiral wire localization of lung nodules: procedure effectiveness and oncological usefulness
Abstract
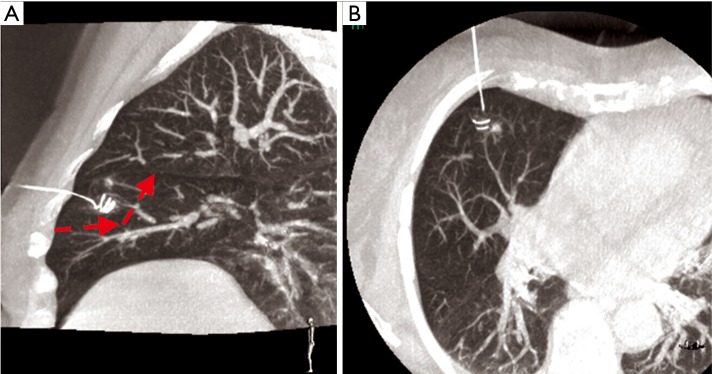
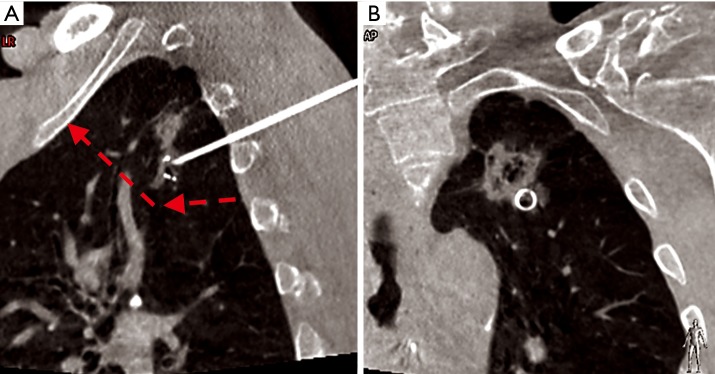
Background: In the last years, a large number of techniques and devices for localizing small pulmonary nodules prior to resection have been developed with the aim of facilitating minimally invasive surgery (VATS). However, each device presents pros and cons and there is no unanimous consensus. We report our experience with an uncommon wire system with spiral shape for percutaneous marking.
Methods: We recorded 102 consecutive CT-guided spiral wire localizations in our Institution, and we evaluated the efficacy of the method according to 4 success rates (SR): (I) successful targeting rate (SR-1): number of successful targeting procedures/number of all localizations; (II) successful localization in operative field (SR-2): (number of successful targeting procedures -number of dislodgements in operative field)/number of all localizations; (III) successful VATS rate (SR-3): number of successful VATS procedures/(number of localizations-number of thoracotomies not due to wire dislocation); (IV) successful curative rate (SR-4): number of neoplastic nodules resected with curative intent with free margins (R0) on definitive tissue diagnosis/number of neoplastic nodules resected with curative intent. Complications rate was recorded as well.
Results: SR-1: 100%, SR-2: 97.1%, SR-3: 100%, SR-4: 100%. Asymptomatic pneumothorax and minimal parenchymal hemorrhage were observed in 5 (4.9%) and 19 (18.6%) cases, respectively.
Conclusions: Spiral wire localization showed very good results in terms of feasibility, stability in operative field and contributed to effective use of VATS during wedge resection performed for malignant nodules. In the era of widespread radiological investigations (as it is happening in lung cancer screening) and evolutions in cancer treatments, this appears to be clinically relevant.
Keywords: Small pulmonary nodules; localization; lung resection; video-assisted thoracic surgery (VATS).
2019 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

Comment in
-
Seeking the holy grail of markers.J Thorac Dis. 2020 Oct;12(10):5259-5261. doi: 10.21037/jtd.2020.04.56. J Thorac Dis. 2020. PMID: 33209358 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous