

Outcomes after total robotic esophagectomy for esophageal cancer: a propensity-matched comparison with hybrid robotic esophagectomy
- PMID: 32030248
- PMCID: PMC6988082
- DOI: 10.21037/jtd.2019.11.58
Outcomes after total robotic esophagectomy for esophageal cancer: a propensity-matched comparison with hybrid robotic esophagectomy
Abstract
Background: Robot-assisted minimally invasive esophagectomy (RAMIE) reduces postoperative respiratory complications and enables meticulous mediastinal lymphadenectomy. However, whether adding a robotic abdominal procedure to a robotic thoracic procedure can result in better outcomes is unclear. We examined outcomes after total-RAMIE (T-RAMIE) and compared them with the outcomes after hybrid-RAMIE (H-RAMIE).
Methods: Total of 227 patients who underwent robotic esophagectomy for esophageal cancer were included. T-RAMIE was defined as esophagectomy performed robotically in both the thoracic and abdominal cavities. Laparotomy was used instead of the robotic procedure in H-RAMIE. T-RAMIE was performed in 144 patients (63.4%), and propensity score matching produced 49 matched pairs from each group. Early and long-term clinical outcomes between the two groups were compared.
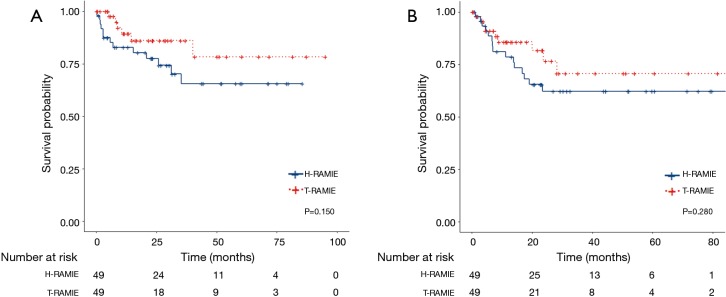
Results: T-RAMIE was mostly performed for upper or mid-thoracic squamous cell carcinoma (n=119, 82.6%) and cervical anastomosis, and three-field lymphadenectomy was performed in 113 (78.5%) and 54 (37.5%) patients, respectively. One laparotomy conversion was necessary because of severe obesity. The propensity-matched analysis demonstrated that T-RAMIE showed a comparable 90-day mortality rate with H-RAMIE (0% vs. 6.1%, P=0.083). The incidence rates of total (63.3% vs. 63.3%; P=1.000), abdominal (8.2% vs. 14.3%; P=0.366), and respiratory complications (10.2% vs. 10.2%; P=1.000) were not different between two groups. The number of harvested abdominal lymph nodes was similar (12.4±9.0 vs. 12.3±8.9; P=0.992). Median follow-up duration for T-RAMIE and H-RAMIE was 16.3 and 23.5 months, respectively. Two-year overall survival rate (86.2% in T-RAMIE vs. 77.6% in H-RAMIE; P=0.150) and recurrence-free survival (76.6% in T-RAMIE vs. 62.2% in H-RAMIE; P=0.280) were comparable between the two groups.
Conclusions: In this matched analysis, T-RAMIE and H-RAMIE showed comparable early outcomes and long-term survival. The low tendencies of early mortality and conversion rate of T-RAMIE suggest that it might be a safe alternative to open stomach mobilization and abdominal lymphadenectomy.
Keywords: Robotic surgery; clinical outcomes; esophageal surgery; minimally invasive surgery.
2019 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Comment in
-
Favorable clinical outcomes of total robotic esophagectomy for esophageal cancer.J Thorac Dis. 2020 Jul;12(7):3455-3456. doi: 10.21037/jtd.2020.03.123. J Thorac Dis. 2020. PMID: 32802420 Free PMC article. No abstract available.
-
Robotic gastric mobilization in robotic minimally invasive esophagectomy.J Thorac Dis. 2020 Jul;12(7):3457-3459. doi: 10.21037/jtd.2020.03.124. J Thorac Dis. 2020. PMID: 32802421 Free PMC article. No abstract available.
-
Robotic surgery facilitates complex minimally invasive operations.J Thorac Dis. 2020 Sep;12(9):4606-4607. doi: 10.21037/jtd-2020-42. J Thorac Dis. 2020. PMID: 33145032 Free PMC article. No abstract available.
References
-
- Nafteux P, Moons J, Coosemans W, et al. Minimally invasive oesophagectomy: a valuable alternative to open oesophagectomy for the treatment of early oesophageal and gastro-oesophageal junction carcinoma. Eur J Cardiothorac Surg 2011;40:1455-65. - PubMed
LinkOut - more resources
Full Text Sources