

The benefits of digital drainage system versus traditional drainage system after robotic-assisted pulmonary lobectomy
- PMID: 32030250
- PMCID: PMC6988061
- DOI: 10.21037/jtd.2019.11.69
The benefits of digital drainage system versus traditional drainage system after robotic-assisted pulmonary lobectomy
Abstract
Background: Postoperative air leaks are the most common complication after a pulmonary resection. There is no data in the literature comparing the traditional and digital chest drainage system after a robotic-assisted pulmonary lobectomy.
Methods: This was a retrospective, correlational study. Medical records from 182 eligible robotic-assisted lobectomy patients were evaluated to determine the association between digital and traditional chest tube drainage systems (CTDS) with postoperative chest tube days, hospital LOS, chest tube reinsertion during hospitalization, and 30-day readmission for pneumothorax. Multiple regression was used to determine the association between CTDS while controlling for confounding variables.
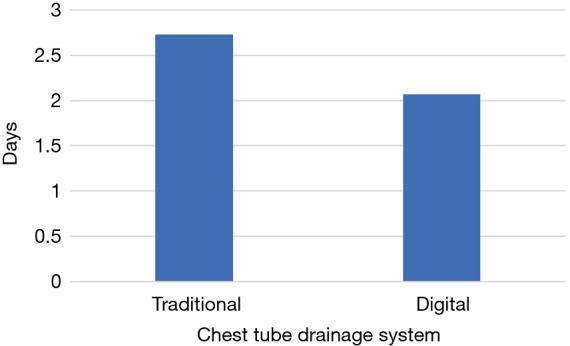
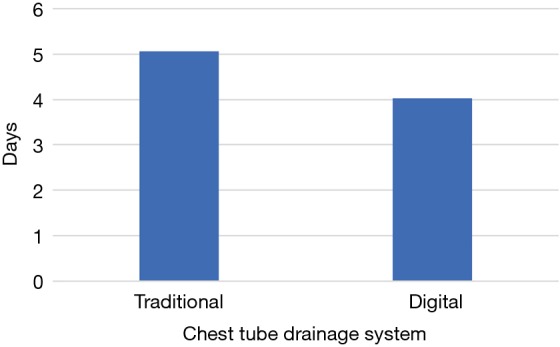
Results: No differences were noted between groups for age, gender, BMI, smoking, adhesions or neoadjuvant therapy. Patients with digital drainage systems had significantly shorter chest tube duration than those with traditional drainage systems (2.07 vs. 2.73 days, P=0.003). After controlling for age and BMI, CTDS was not found to be a significant predictor of CT duration. Digital drainage system were also associated with significantly shorter hospital LOS (4.02 vs. 5.06 days, P=0.01) After controlling for age, BMI, and presence of post-op a-fib, use of a digital CTDS was significantly associated with 1 day shorter hospital LOS. Chest tube reinsertion occurred four times more frequently with traditional drainage systems, but the difference did not achieve the level of statistical significance (P=0.059). The frequency of readmission due to pneumothorax was very low (1 patient per group), which prevented comparative statistical analysis.
Conclusions: In the digital drainage system there are shorter chest tube days and hospital length of stay after a robotic-assisted lobectomy. The decision to remove chest tubes in the traditional drainage system is burdened with uncertainty. The digital drainage system reduces intraobserver variability allowing for improved decision making in chest tube removal. Both CT duration and hospital LOS were shorter using unadjusted analyses. Type of CTDS was not significantly associated with CT duration after controlling for age and BMI. However, after controlling for age, BMI, and post-op atrial fibrillation, use of the digital CTDS was associated with a 1 day reduction in hospital LOS.
Keywords: Digital drainage system; air leak; lobectomy; robotic-assisted thoracoscopic surgery.
2019 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Comment in
-
Digital chest drainage systems are beneficial for robotic-assisted lung resections.J Thorac Dis. 2020 Jun;12(6):2991-2992. doi: 10.21037/jtd.2020.03.107. J Thorac Dis. 2020. PMID: 32642215 Free PMC article. No abstract available.
-
Digital chest drainage vs. water seal chest drainage in the robotic era.J Thorac Dis. 2020 Jun;12(6):3004-3006. doi: 10.21037/jtd.2020.03.86. J Thorac Dis. 2020. PMID: 32642219 Free PMC article. No abstract available.
-
Objective analysis of postoperative air leaks can aid in decision-making, but does the use of digital drains really impact patient outcomes?J Thorac Dis. 2020 Aug;12(8):3927-3929. doi: 10.21037/jtd.2020.04.22. J Thorac Dis. 2020. PMID: 32944301 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources
Miscellaneous