

Association between uric acid levels and cardio-renal outcomes and death in patients with type 2 diabetes: A subanalysis of EMPA-REG OUTCOME
- PMID: 32030863
- PMCID: PMC7317186
- DOI: 10.1111/dom.13991
Association between uric acid levels and cardio-renal outcomes and death in patients with type 2 diabetes: A subanalysis of EMPA-REG OUTCOME
Abstract
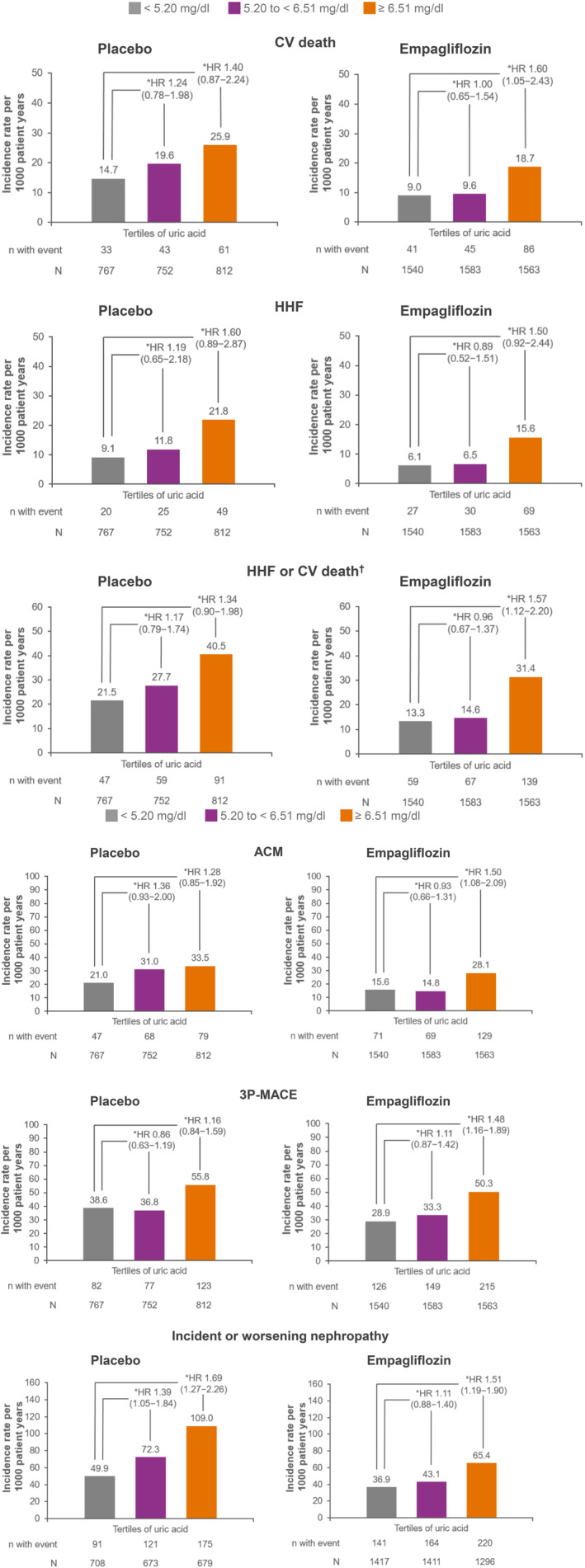
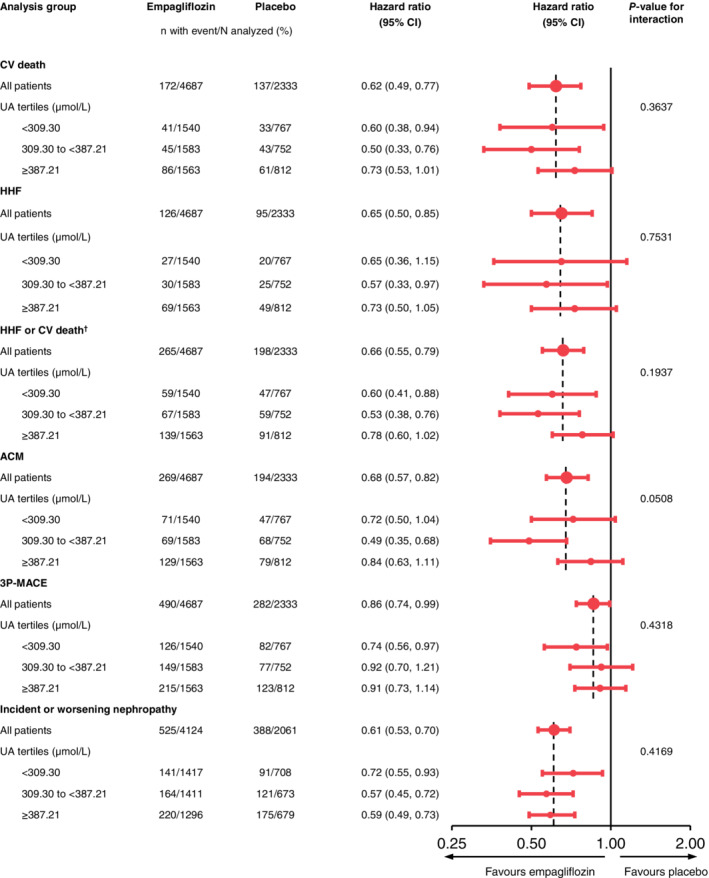
In the EMPA-REG OUTCOME trial, we explored the association between pre-randomization uric acid level tertile (<309.30 μmol/L; 309.30 to <387.21 μmol/L; ≥387.21 μmol/L) and cardiovascular (CV) death, hospitalization for heart failure (HHF), HHF or CV death, all-cause mortality, three-point major adverse CV events (MACE), and incident or worsening nephropathy. Patients with type 2 diabetes and CV disease received empagliflozin or placebo. The median baseline plasma uric acid level was 344.98 μmol/L, and patients' baseline characteristics were mainly balanced across tertiles. Baseline uric acid levels were associated with cardio-renal outcomes: in the placebo group, for the highest versus lowest tertile, the multivariable hazard ratios for three-point MACE, HHF or CV death, and incident or worsening nephropathy were 1.22 (95% confidence interval [CI] 0.89-1.67; P = 0.2088), 1.51 (95% CI 1.02-2.23; P = 0.0396) and 1.77 (95% CI 1.33-2.34; P < 0.0001), respectively. When tested as a continuous variable, baseline uric acid was associated with all outcomes in the placebo group. Empagliflozin improved all cardio-renal outcomes across tertiles, with all interaction P values >0.05. Further investigation of these relationships is required.
Keywords: SGLT2 inhibitor; cardiovascular disease; clinical trial; empagliflozin; type 2 diabetes.
© 2020 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
S.V. is President of the Canadian Medical and Surgical Knowledge Translation Research Group, a federally incorporated not‐for‐profit physician organization, holds a Tier 1 Canada Research Chair in Cardiovascular Surgery, and has received research grants and/or speaking honoraria from Boehringer Ingelheim/Eli Lilly and Company, AstraZeneca, Janssen, Merck, Novartis, Novo Nordisk, Amgen, Sanofi, Servier, Valeant, Bayer and Pfizer. Q.J. has received travel support as an advisory board member from Merck & Co., Inc for the STRATEGY study, and has attended advisory boards and been a speaker for Eli Lilly, Novo Nordisk, Merck Sharp & Dohme China, Sanofi Aventis, Huadong Pharmaceuticals Company and Medtronic, and received research grants from Novo Nordisk, Merck Sharp & Dohme China and AstraZeneca. D.L.B. discloses the following relationships: Advisory Board: Cardax, Cereno Scientific, Elsevier Practice Update Cardiology, Medscape Cardiology, PhaseBio, PLx Pharma, Regado Biosciences; Board of Directors: Boston VA Research Institute, Society of Cardiovascular Patient Care, TobeSoft; Chair: American Heart Association Quality Oversight Committee; Data Monitoring Committees: Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial, funded by St. Jude Medical, now Abbott), Cleveland Clinic (including for the ExCEED trial, funded by Edwards), Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGE trial, funded by Daiichi Sankyo), Population Health Research Institute; Honoraria: American College of Cardiology (Senior Associate Editor, Clinical Trials and News,
Figures
References
-
- Ndrepepa G. Uric acid and cardiovascular disease. Clin Chim Acta. 2018;484:150‐163. - PubMed
-
- Bailey CJ. Uric acid and the cardio‐renal effects of SGLT2 inhibitors. Diabetes Obes Metab. 2019;21:1291‐1298. - PubMed
-
- Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med. 2015;373:2117‐2128. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
