

Preoperative Cognitive Abnormality, Intraoperative Electroencephalogram Suppression, and Postoperative Delirium: A Mediation Analysis
- PMID: 32032096
- PMCID: PMC7228853
- DOI: 10.1097/ALN.0000000000003181
Preoperative Cognitive Abnormality, Intraoperative Electroencephalogram Suppression, and Postoperative Delirium: A Mediation Analysis
Abstract
Background: Postoperative delirium is a common complication that hinders recovery after surgery. Intraoperative electroencephalogram suppression has been linked to postoperative delirium, but it is unknown if this relationship is causal or if electroencephalogram suppression is merely a marker of underlying cognitive abnormalities. The hypothesis of this study was that intraoperative electroencephalogram suppression mediates a nonzero portion of the effect between preoperative abnormal cognition and postoperative delirium.
Methods: This is a prespecified secondary analysis of the Electroencephalography Guidance of Anesthesia to Alleviate Geriatric Syndromes (ENGAGES) randomized trial, which enrolled patients age 60 yr or older undergoing surgery with general anesthesia at a single academic medical center between January 2015 and May 2018. Patients were randomized to electroencephalogram-guided anesthesia or usual care. Preoperative abnormal cognition was defined as a composite of previous delirium, Short Blessed Test cognitive score greater than 4 points, or Eight Item Interview to Differentiate Aging and Dementia score greater than 1 point. Duration of intraoperative electroencephalogram suppression was defined as number of minutes with suppression ratio greater than 1%. Postoperative delirium was detected via Confusion Assessment Method or chart review on postoperative days 1 to 5.
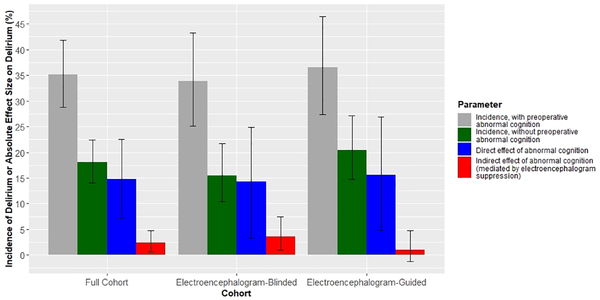
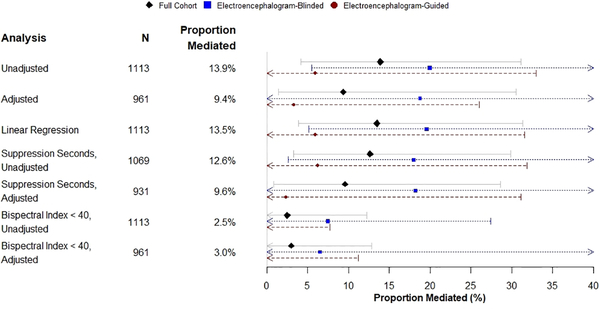
Results: Among 1,113 patients, 430 patients showed evidence of preoperative abnormal cognition. These patients had an increased incidence of postoperative delirium (151 of 430 [35%] vs.123 of 683 [18%], P < 0.001). Of this 17.2% total effect size (99.5% CI, 9.3 to 25.1%), an absolute 2.4% (99.5% CI, 0.6 to 4.8%) was an indirect effect mediated by electroencephalogram suppression, while an absolute 14.8% (99.5% CI, 7.2 to 22.5%) was a direct effect of preoperative abnormal cognition. Randomization to electroencephalogram-guided anesthesia did not change the mediated effect size (P = 0.078 for moderation).
Conclusions: A small portion of the total effect of preoperative abnormal cognition on postoperative delirium was mediated by electroencephalogram suppression. Study precision was too low to determine if the intervention changed the mediated effect.
Conflict of interest statement
Figures


References
-
- Lat I, McMillian W, Taylor S, Janzen JM, Papadopoulos S, Korth L, Ehtisham A, Nold J, Agarwal S, Azocar R, Burke P: The impact of delirium on clinical outcomes in mechanically ventilated surgical and trauma patients. Crit Care Med 2009; 37:1898–905 - PubMed
-
- Edelstin DM, Aharonoff GB, Karp A, Capla EL, Zuckerman JD, Koval KJ: Effect of postoperative delirium on outcome after hip fracture. Clin Orthop Relat Res 2004; 422:195–200 - PubMed
-
- Bickel H, Gradinger R, Kochs E, Förstl H: High risk of cognitive and functional decline after postoperative delirium. Dement Geriatr Cogn Disord 2008; 26:26–31 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
