

Identification of Pediatric Sepsis for Epidemiologic Surveillance Using Electronic Clinical Data
- PMID: 32032262
- PMCID: PMC7008717
- DOI: 10.1097/PCC.0000000000002170
Identification of Pediatric Sepsis for Epidemiologic Surveillance Using Electronic Clinical Data
Abstract
Objectives: A method to identify pediatric sepsis episodes that is not affected by changing diagnosis and claims-based coding practices does not exist. We derived and validated a surveillance algorithm to identify pediatric sepsis using routine clinical data and applied the algorithm to study longitudinal trends in sepsis epidemiology.
Design: Retrospective observational study.
Setting: Single academic children's hospital.
Patients: All emergency and hospital encounters from January 2011 to January 2019, excluding neonatal ICU and cardiac center.
Exposure: Sepsis episodes identified by a surveillance algorithm using clinical data to identify infection and concurrent organ dysfunction.
Interventions: None.
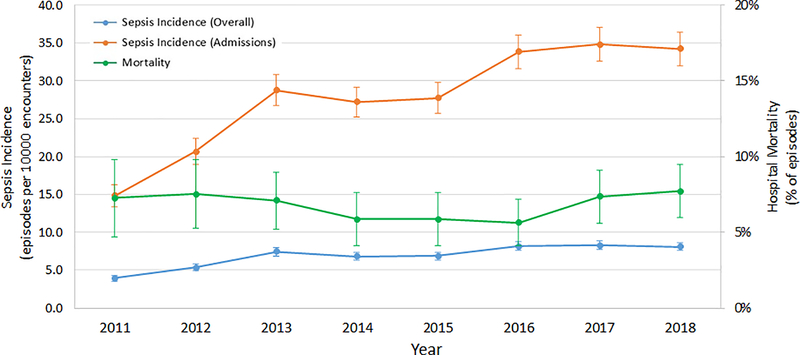
Measurements and main results: A surveillance algorithm was derived and validated in separate cohorts with suspected sepsis after clinician-adjudication of final sepsis diagnosis. We then applied the surveillance algorithm to determine longitudinal trends in incidence and mortality of pediatric sepsis over 8 years. Among 93,987 hospital encounters and 1,065 episodes of suspected sepsis in the derivation period, the surveillance algorithm yielded sensitivity 78% (95% CI, 72-84%), specificity 76% (95% CI, 74-79%), positive predictive value 41% (95% CI, 36-46%), and negative predictive value 94% (95% CI, 92-96%). In the validation period, the surveillance algorithm yielded sensitivity 84% (95% CI, 77-92%), specificity of 65% (95% CI, 59-70%), positive predictive value 43% (95% CI, 35-50%), and negative predictive value 93% (95% CI, 90-97%). Notably, most "false-positives" were deemed clinically relevant sepsis cases after manual review. The hospital-wide incidence of sepsis was 0.69% (95% CI, 0.67-0.71%), and the inpatient incidence was 2.8% (95% CI, 2.7-2.9%). Risk-adjusted sepsis incidence, without bias from changing diagnosis or coding practices, increased over time (adjusted incidence rate ratio per year 1.07; 95% CI, 1.06-1.08; p < 0.001). Mortality was 6.7% and did not change over time (adjusted odds ratio per year 0.98; 95% CI, 0.93-1.03; p = 0.38).
Conclusions: An algorithm using routine clinical data provided an objective, efficient, and reliable method for pediatric sepsis surveillance. An increased sepsis incidence and stable mortality, free from influence of changes in diagnosis or billing practices, were evident.
Figures
Comment in
-
Grappling With Real-Time Diagnosis and Public Health Surveillance in Sepsis: Can Clinical Data Provide the Answer?Pediatr Crit Care Med. 2020 Feb;21(2):196-197. doi: 10.1097/PCC.0000000000002212. Pediatr Crit Care Med. 2020. PMID: 32032265 No abstract available.
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001;29(7):1303–1310. - PubMed
-
- Hartman ME, Linde-Zwirble WT, Angus DC, et al. Trends in the Epidemiology of Pediatric Severe Sepsis. Pediatr Crit Care Med 2013;14(7):868–693. - PubMed
-
- Goldstein B, Giroir B, Randolph A. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med 2005;6(1):2–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
