

The Role of Radiotherapy for Chordoma Patients Managed With Surgery: Analysis of the National Cancer Database
- PMID: 32032324
- PMCID: PMC7649561
- DOI: 10.1097/BRS.0000000000003406
The Role of Radiotherapy for Chordoma Patients Managed With Surgery: Analysis of the National Cancer Database
Abstract
Study design: Retrospective review.
Objective: To determine if adjuvant radiation therapy (RT) improves overall survival (OS) following surgical resection of chordomas.
Summary of background data: The role of RT for the treatment of chordomas remains incompletely described. Previous studies have not found adjuvant RT to improve OS, but these studies did not group patients based on surgical margin status or radiation dose or modality. We used the National Cancer Database to investigate the role of RT in chordomas following surgical resection.
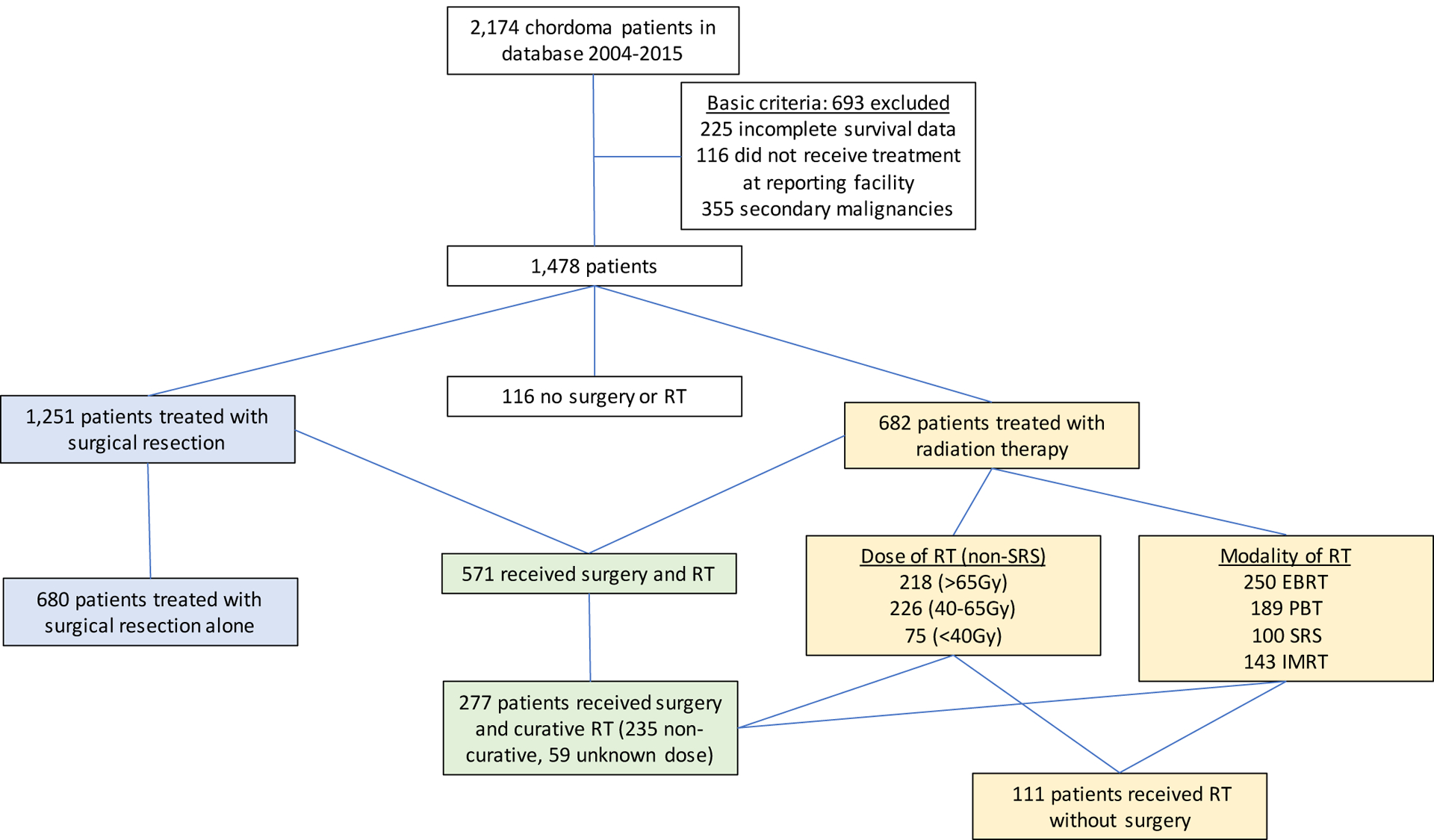
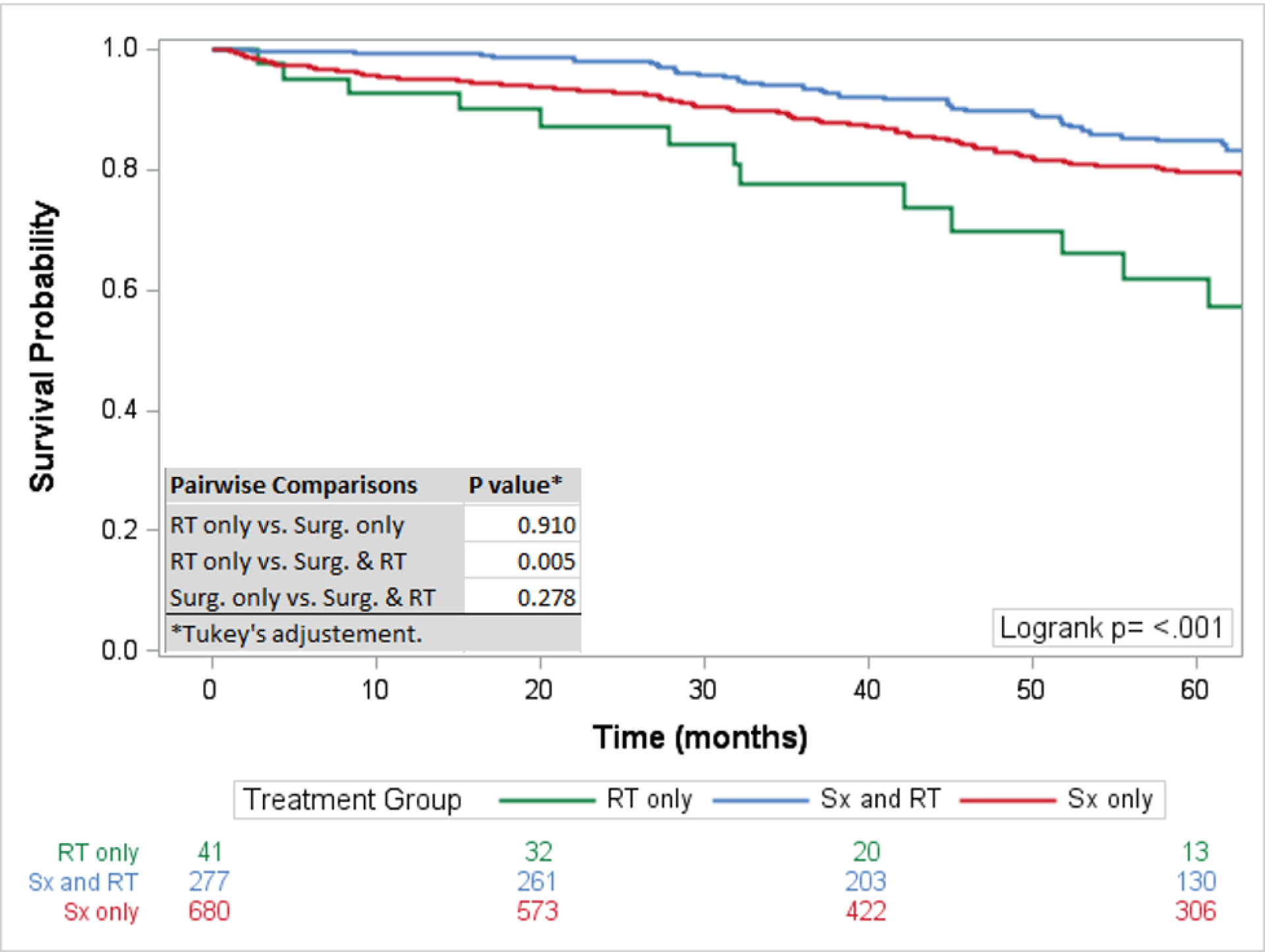
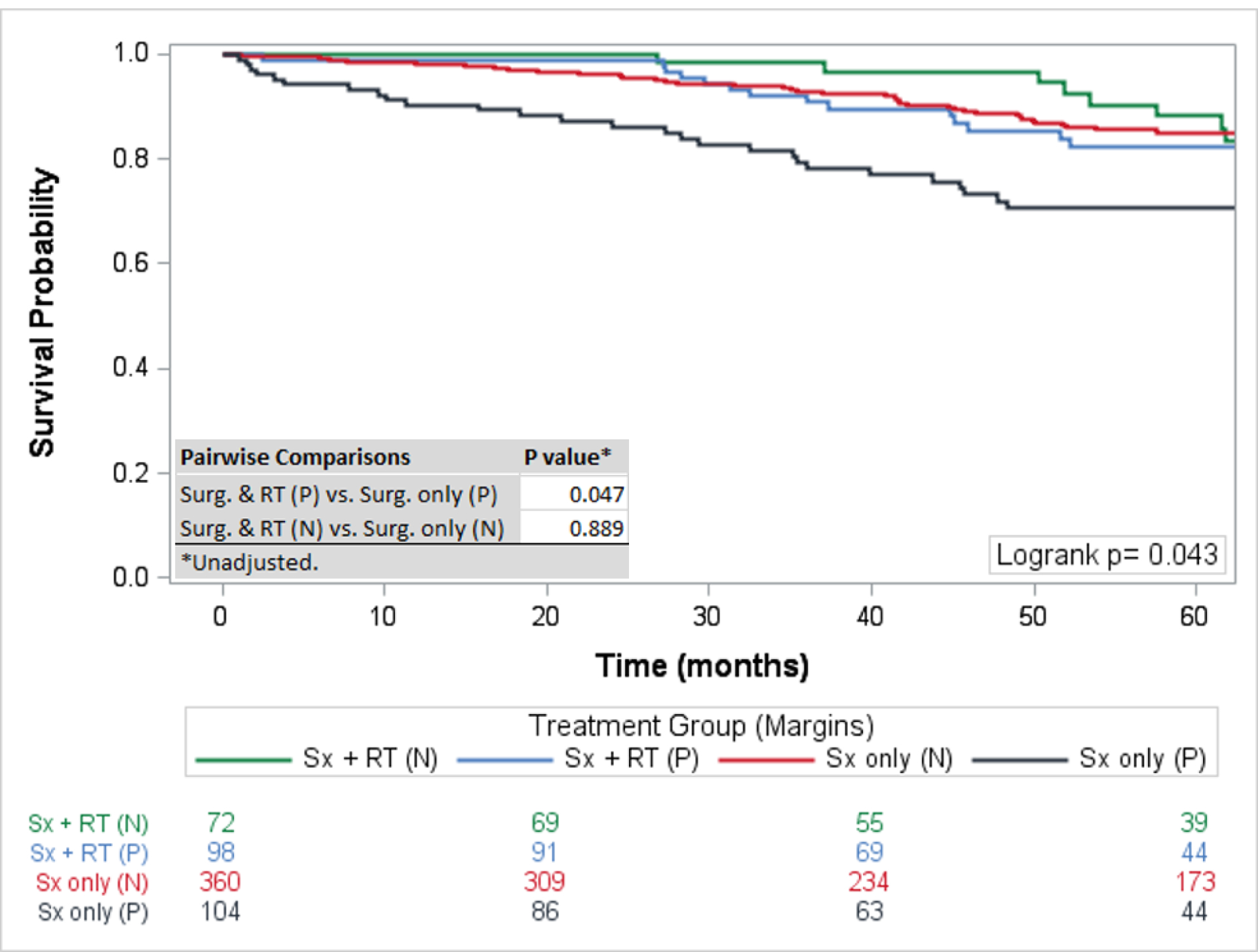
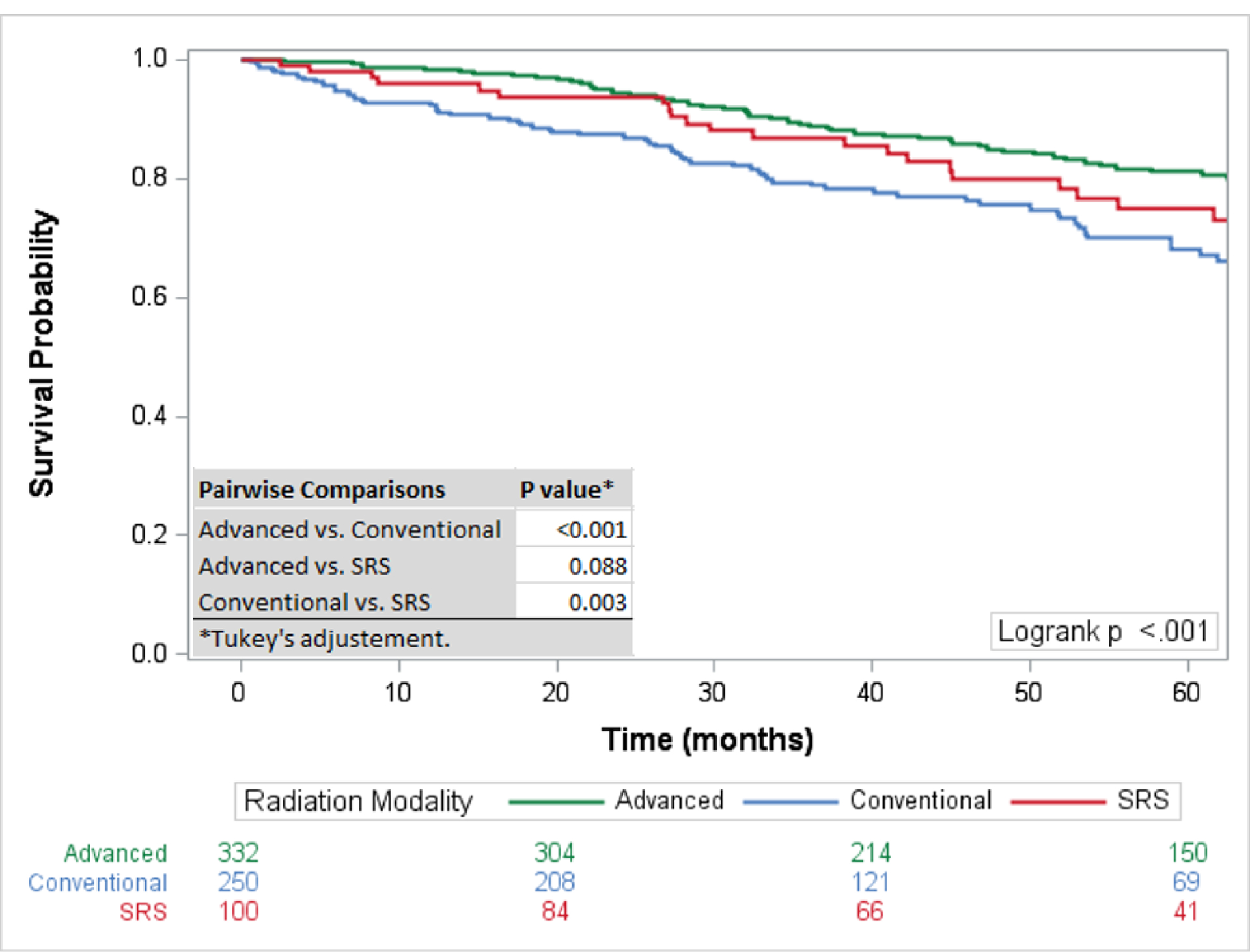
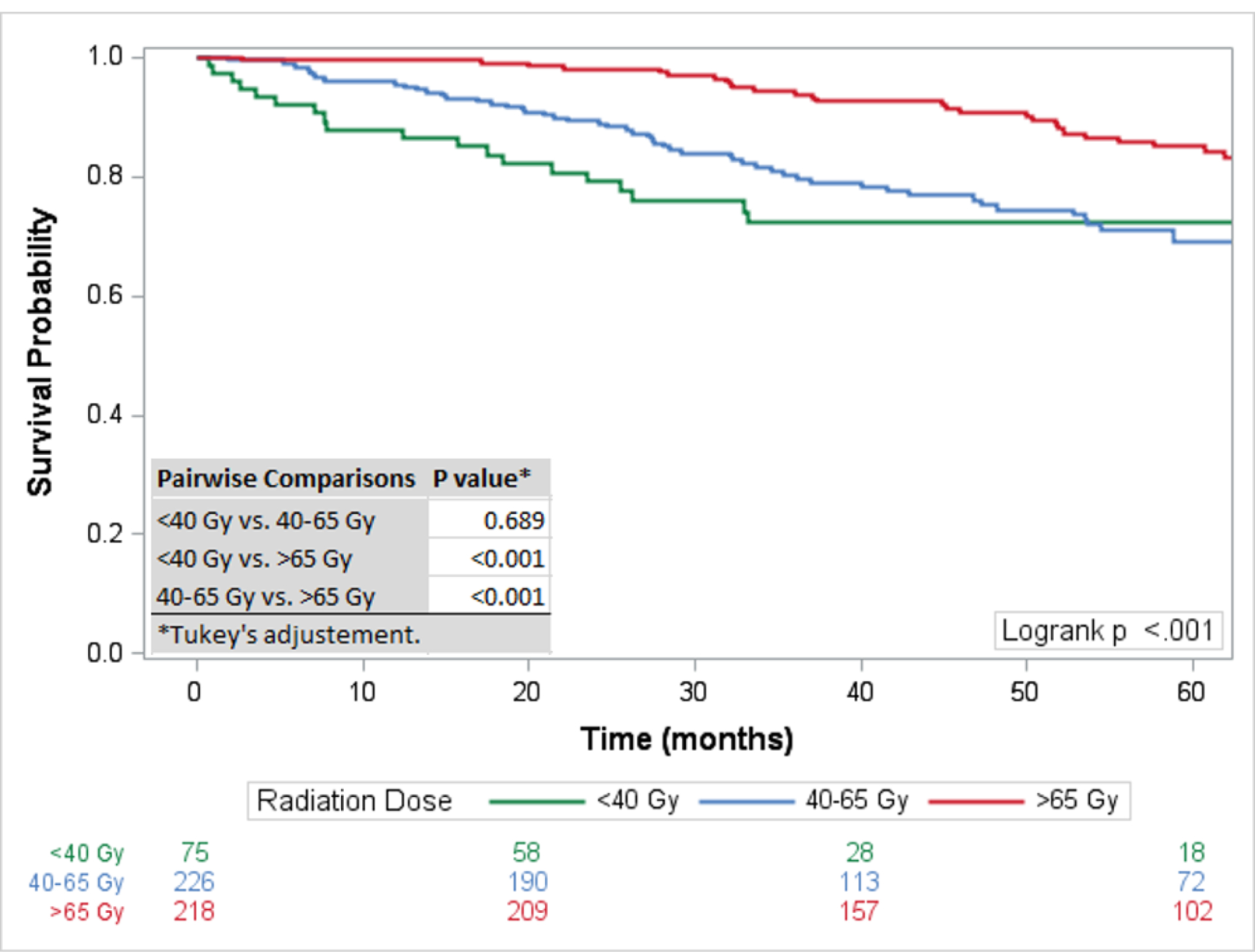
Methods: Patients were stratified based on surgical margin status (positive vs. negative). Utilizing the Kaplan-Meier method, OS was compared between treatment modalities (surgical resection alone, therapeutic RT alone, and surgical resection plus therapeutic RT). OS was subsequently compared between patients treated with palliative dose (<40 Gy), low dose (40-65 Gy), and high dose (>65 Gy) RT. Similarly, OS was compared between advanced RT modalities including proton beam therapy (PBT) and intensity-modulated radiation therapy (IMRT), stereotactic radiosurgery (SRS), and external beam radiation therapy (EBRT). A multivariable model was used to determine adjusted variables predictive of mortality.
Results: One thousand four hundred seventy eight chordoma patients were identified; skull base (n = 567), sacral (n = 551), and mobile spine (n = 360). Surgical resection and therapeutic adjuvant RT improved 5-year survival in patients with positive surgical margins (82% vs. 71%, P = 0.03). No clear survival benefit was observed with the addition of adjuvant RT in patients with negative surgical margins. High dose RT was associated with improved OS compared with palliative and low dose RT (P < 0.001). Advanced RT techniques and SRS were associated with improved OS compared with EBRT. In the multivariate analysis high dose advanced RT (>65 Gy) was superior to EBRT.
Conclusion: Patients with positive surgical margins benefit from adjuvant RT. Optimal OS is associated with adjuvant RT administered with advanced techniques and cumulative dose more than 65 Gy.
Level of evidence: 4.
Figures
References
-
- Walcott BP, Nahed BV, Mohyeldin A, et al. Chordoma: current concepts, management, and future directions. The Lancet Oncology. 2012;13(2):e69–76. - PubMed
-
- Lee IJ, Lee RJ, Fahim DK. Prognostic Factors and Survival Outcome in Patients with Chordoma in the United States: A Population-Based Analysis. World neurosurgery. 2017;104:346–55. - PubMed
-
- Dea N, Fisher CG, Reynolds JJ, et al. Current treatment strategy for newly diagnosed chordoma of the mobile spine and sacrum: results of an international survey. Journal of neurosurgery Spine. 2018;30(1):119–25. - PubMed
-
- Sun HH, Hong X, Liu B, et al. Survival analysis of patients with spinal chordomas. Neurosurgical review. 2018. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
