

Point-of-care oral cytology tool for the screening and assessment of potentially malignant oral lesions
- PMID: 32032477
- PMCID: PMC7078980
- DOI: 10.1002/cncy.22236
Point-of-care oral cytology tool for the screening and assessment of potentially malignant oral lesions
Abstract
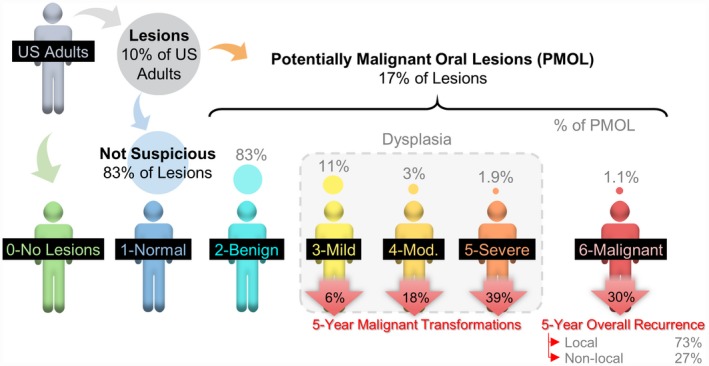
Background: The effective detection and monitoring of potentially malignant oral lesions (PMOL) are critical to identifying early-stage cancer and improving outcomes. In the current study, the authors described cytopathology tools, including machine learning algorithms, clinical algorithms, and test reports developed to assist pathologists and clinicians with PMOL evaluation.
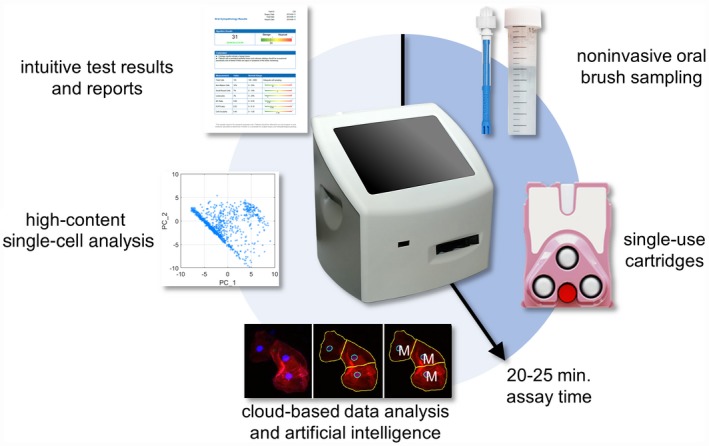
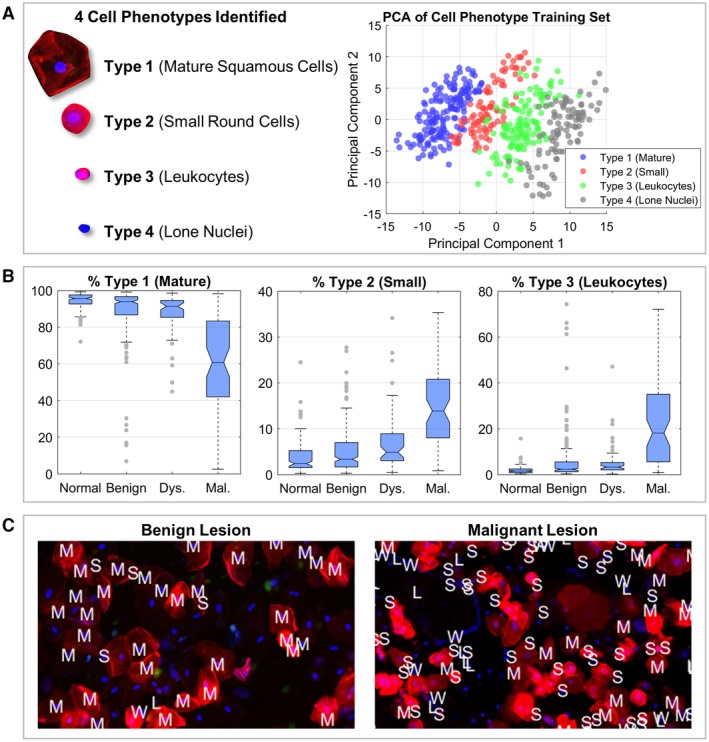
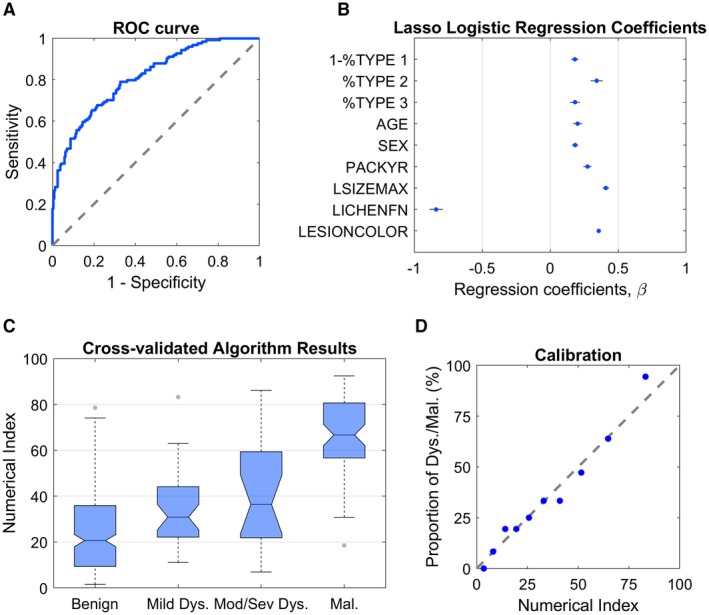
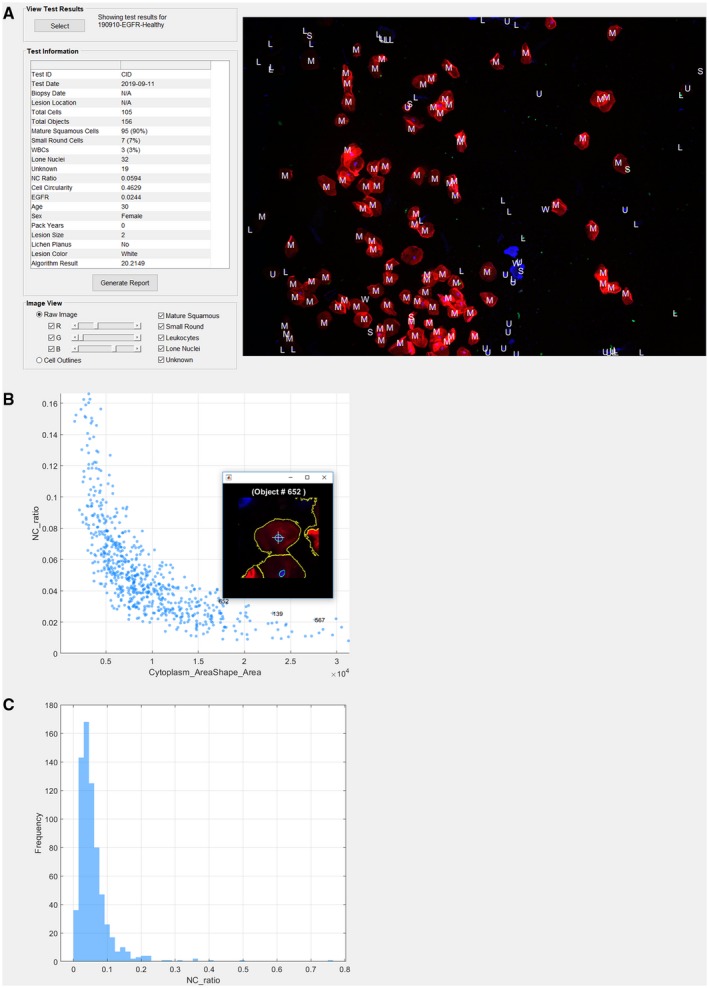
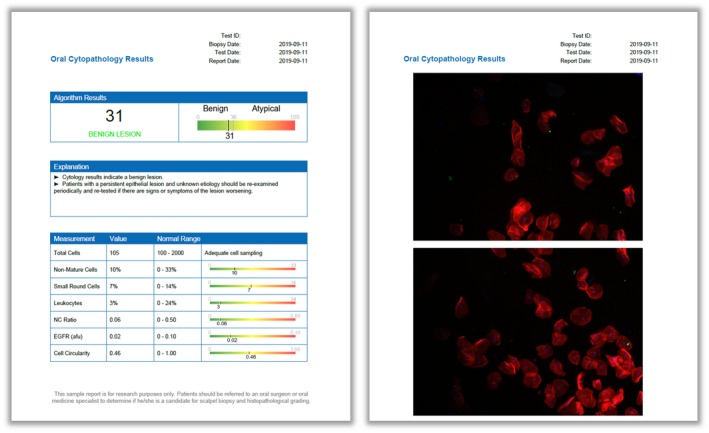
Methods: Data were acquired from a multisite clinical validation study of 999 subjects with PMOLs and oral squamous cell carcinoma (OSCC) using a cytology-on-a-chip approach. A machine learning model was trained to recognize and quantify the distributions of 4 cell phenotypes. A least absolute shrinkage and selection operator (lasso) logistic regression model was trained to distinguish PMOLs and cancer across a spectrum of histopathologic diagnoses ranging from benign, to increasing grades of oral epithelial dysplasia (OED), to OSCC using demographics, lesion characteristics, and cell phenotypes. Cytopathology software was developed to assist pathologists in reviewing brush cytology test results, including high-content cell analyses, data visualization tools, and results reporting.
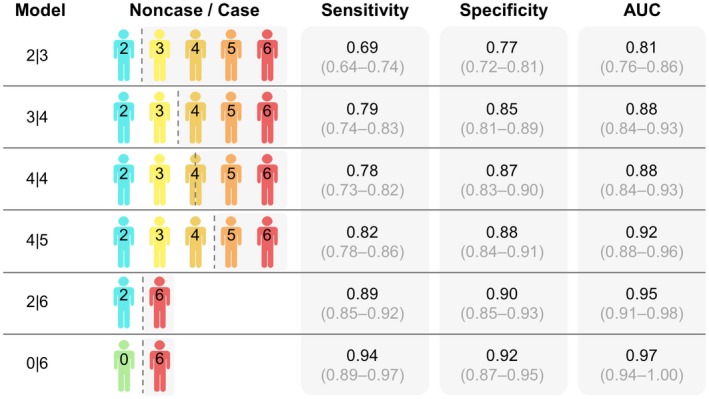
Results: Cell phenotypes were determined accurately through an automated cytological assay and machine learning approach (99.3% accuracy). Significant differences in cell phenotype distributions across diagnostic categories were found in 3 phenotypes (type 1 ["mature squamous"], type 2 ["small round"], and type 3 ["leukocytes"]). The clinical algorithms resulted in acceptable performance characteristics (area under the curve of 0.81 for benign vs mild dysplasia and 0.95 for benign vs malignancy).
Conclusions: These new cytopathology tools represent a practical solution for rapid PMOL assessment, with the potential to facilitate screening and longitudinal monitoring in primary, secondary, and tertiary clinical care settings.
Keywords: artificial intelligence; biomarkers; cytology; oral epithelial dysplasia; point-of-care testing; single-cell analysis; squamous cell carcinoma.
© 2020 The Authors. Cancer Cytopathology published by Wiley Periodicals, Inc. on behalf of American Cancer Society.
Conflict of interest statement
Michael P. McRae has served as paid consultant for SensoDx and has a provisional patent pending. Glennon W. Simmons has patents US10060937B2 and US7781226B2 issued. Denise A. Trochesset has received grants from the New York University College of Dentistry for work performed as part of the current study. Martin H. Thornhill has received National Institutes of Health grant 1RC2DE020785‐01 for work performed as part of the current study. Spencer W. Redding has patent US9535068B2 issued. Stella K. Kang has received royalties from Wolters Kluwer for work performed outside of the current study. John T. McDevitt has received grants from the National Institutes of Health for work performed as part of the current study (grants 1RC2DE020785‐01, 4R44DE025798‐02, and R01DE024392) and has a provisional patent pending. In addition, he has an ownership position and an equity interest in SensoDx II LLC and also serves on its Scientific Advisory Board. The other authors made no disclosures.
Figures
References
-
- Shield KD, Ferlay J, Jemal A, et al. The global incidence of lip, oral cavity, and pharyngeal cancers by subsite in 2012. CA Cancer J Clin. 2017;67:51‐64. - PubMed
-
- National Cancer Institute Surveillance, Epidemiology, and End Results Program . Cancer stat facts: oral cancer and pharynx cancer. Accessed May 10, 2019. https://seer.cancer.gov/statfacts/html/oralcav.html
-
- Neville BW, Damm DD, Allen CM, Chi AC. Epithelial pathology In: Neville BW, Damm DD, Allen CM, Chi AC, eds. Oral Maxillofacial Pathology. 4th ed Elsevier Health Sciences; 2015:331‐421.
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7‐30. - PubMed
-
- Huber MA. Adjunctive diagnostic techniques for oral and oropharyngeal cancer discovery. Dent Clin North Am. 2018;62:59‐75. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
