

Early Detection of Hyperprogressive Disease in Non-Small Cell Lung Cancer by Monitoring of Systemic T Cell Dynamics
- PMID: 32033028
- PMCID: PMC7073153
- DOI: 10.3390/cancers12020344
Early Detection of Hyperprogressive Disease in Non-Small Cell Lung Cancer by Monitoring of Systemic T Cell Dynamics
Abstract
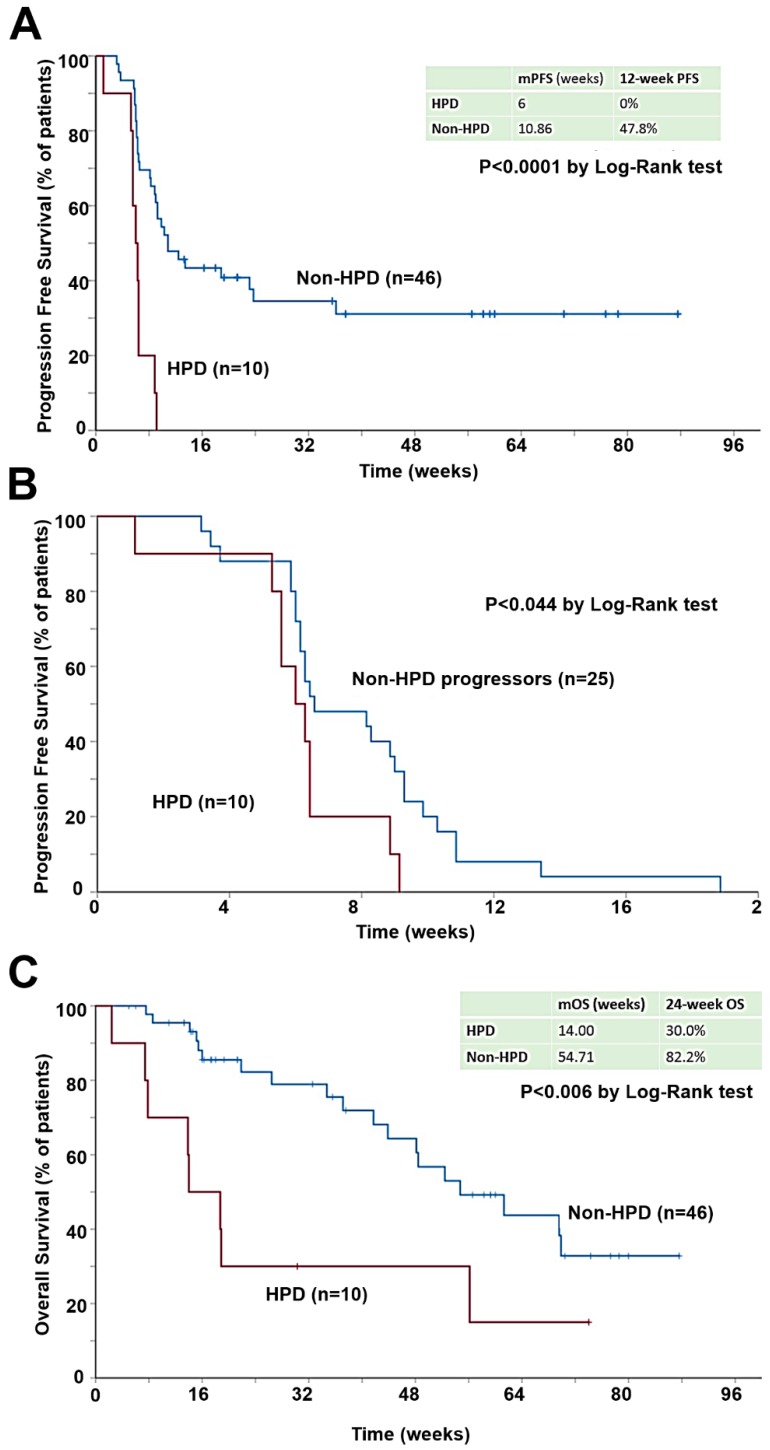
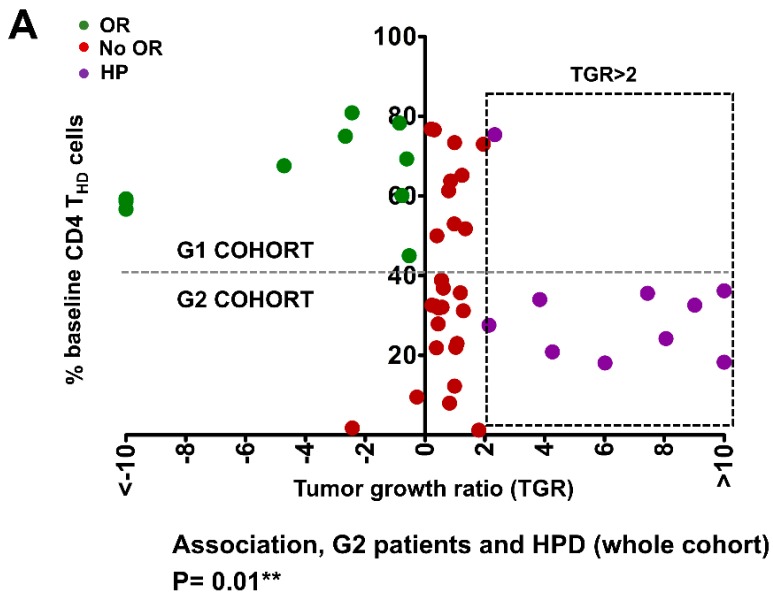
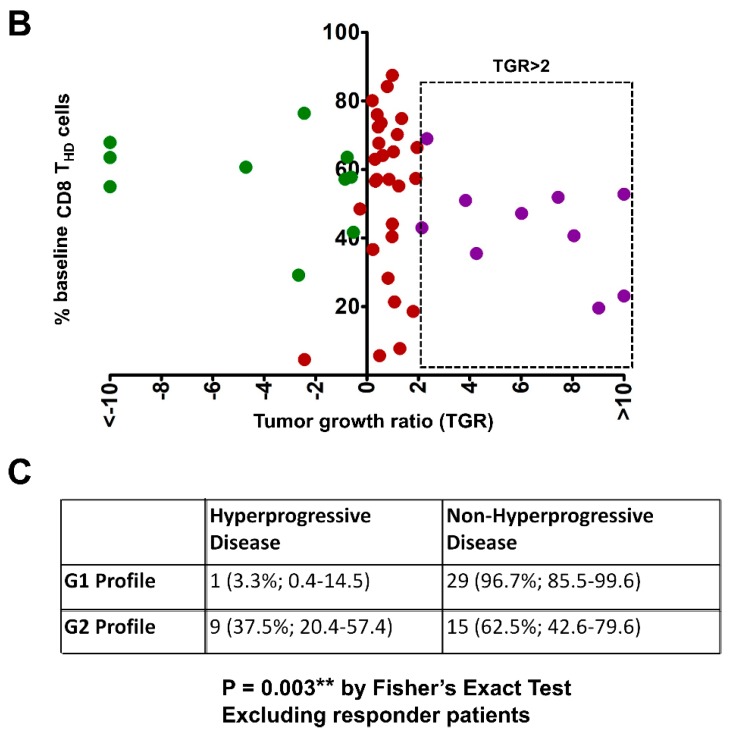
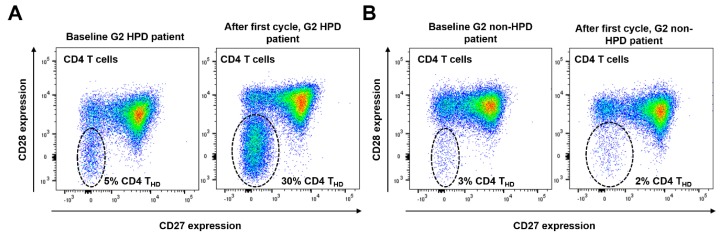
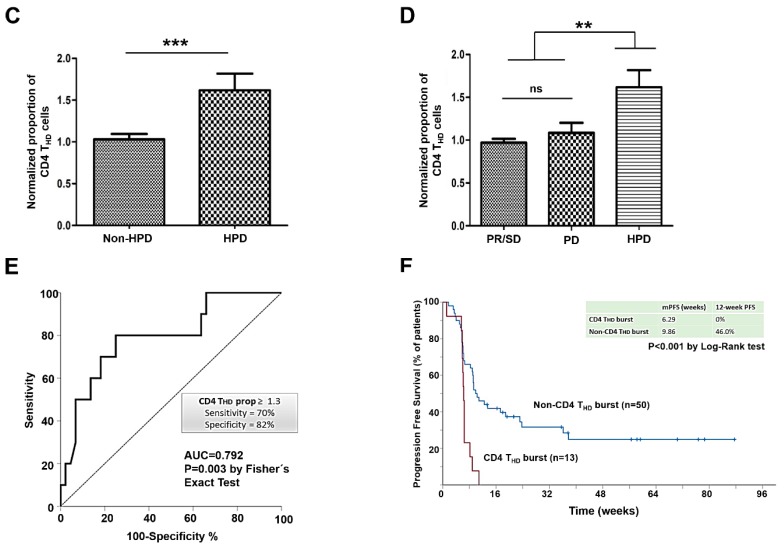
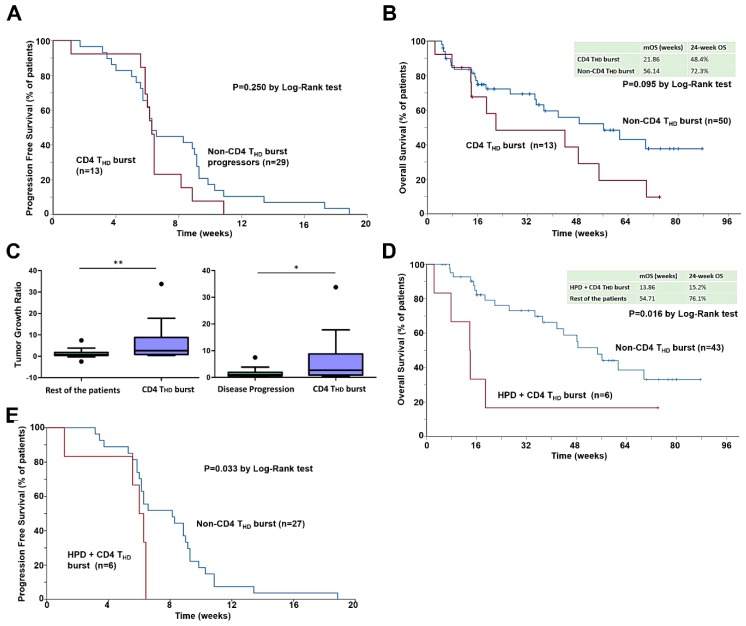
Hyperprogressive disease (HPD) is an adverse outcome of immunotherapy consisting of an acceleration of tumor growth associated with prompt clinical deterioration. The definitions based on radiological evaluation present important technical limitations. No biomarkers have been identified yet. In this study, 70 metastatic NSCLC patients treated with anti-PD-1/PD-L1 immunotherapy after progression to platinum-based therapy were prospectively studied. Samples from peripheral blood were obtained before the first (baseline) and second cycles of treatment. Peripheral blood mononuclear cells (PBMCs) were isolated and differentiation stages of CD4 lymphocytes quantified by flow cytometry and correlated with HPD as identified with radiological criteria. A strong expansion of highly differentiated CD28- CD4 T lymphocytes (CD4 THD) between the first and second cycle of therapy was observed in HPD patients. After normalizing, the proportion of posttreatment/pretreatment CD4 THD was significantly higher in HPD when compared with the rest of patients (median 1.525 vs. 0.990; p = 0.0007), and also when stratifying by HPD, non-HPD progressors, and responders (1.525, 1.000 and 0.9700 respectively; p = 0.0025). A cut-off value of 1.3 identified HPD with 82% specificity and 70% sensitivity. An increase of CD28- CD4 T lymphocytes ≥ 1.3 (CD4 THD burst) was significantly associated with HPD (p = 0.008). The tumor growth ratio (TGR) was significantly higher in patients with expansion of CD4 THD burst compared to the rest of patients (median 2.67 vs. 0.86, p = 0.0049), and also when considering only progressors (median 2.67 vs. 1.03, p = 0.0126). A strong expansion of CD28- CD4 lymphocytes in peripheral blood within the first cycle of therapy is an early differential feature of HPD in NSCLC treated with immune-checkpoint inhibitors. The monitoring of T cell dynamics allows the early detection of this adverse outcome in clinical practice and complements radiological evaluation.
Keywords: NSCLC; hyperprogressive disease; immunotherapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Champiat S., Dercle L., Ammari S., Massard C., Hollebecque A., Postel-Vinay S., Chaput N., Eggermont A., Marabelle A., Soria J.C., et al. Hyperprogressive Disease Is a New Pattern of Progression in Cancer Patients Treated by Anti-PD-1/PD-L1. Clin. Cancer Res. 2017;23:1920–1928. doi: 10.1158/1078-0432.CCR-16-1741. - DOI - PubMed
-
- Saada-Bouzid E., Defaucheux C., Karabajakian A., Coloma V.P., Servois V., Paoletti X., Even C., Fayette J., Guigay J., Loirat D., et al. Hyperprogression during anti-PD-1/PD-L1 therapy in patients with recurrent and/or metastatic head and neck squamous cell carcinoma. Ann. Oncol. 2017;28:1605–1611. doi: 10.1093/annonc/mdx178. - DOI - PubMed
-
- Lo Russo G., Moro M., Sommariva M., Cancila V., Boeri M., Centonze G., Ferro S., Ganzinelli M., Gasparini P., Huber V., et al. Antibody-Fc/FcR Interaction on Macrophages as a Mechanism for Hyperprogressive Disease in Non-small Cell Lung Cancer Subsequent to PD-1/PD-L1 Blockade. Clin. Cancer Res. 2019;25:989–999. doi: 10.1158/1078-0432.CCR-18-1390. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
