

Diagnosing peritoneal tuberculosis
- PMID: 32033999
- PMCID: PMC7035809
- DOI: 10.1136/bcr-2019-233131
Diagnosing peritoneal tuberculosis
Abstract
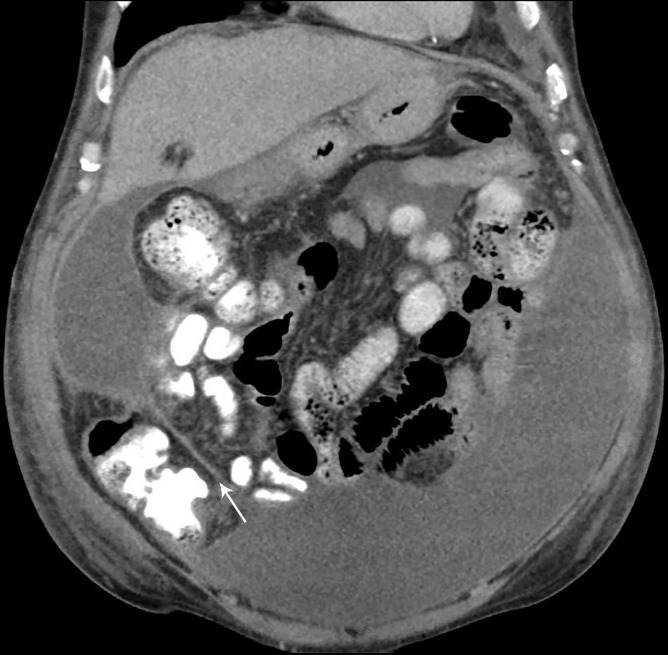
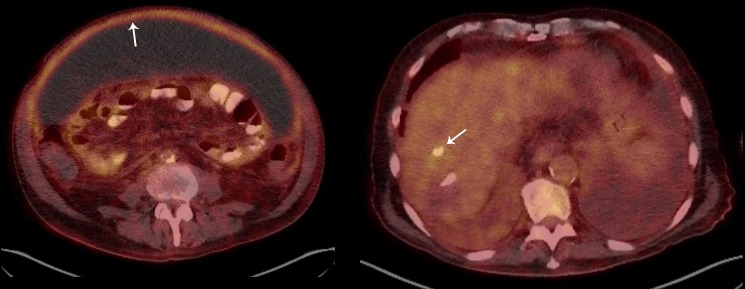
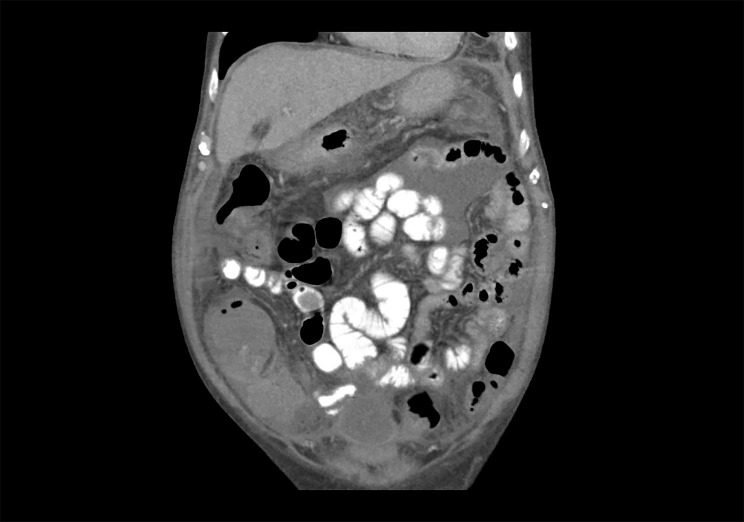
Peritoneal tuberculosis (TB) is one of the most challenging forms of extrapulmonary tuberculosis to diagnose. This challenge can be compounded in low incidence regions, and in patients with cirrhosis in whom the presence of ascites alone may not prompt further investigation. A delay in the diagnosis and treatment of peritoneal tuberculosis may lead to worse clinical outcomes. This case describes a 64-year-old Italian male with decompensated cirrhosis being evaluated for liver transplantation, who developed abdominal pain and a persistent inflammatory ascites with peritoneal thickening despite antibiotic therapy. Peritoneal tuberculosis was suspected, although non-invasive and invasive direct mycobacterial testing remained negative. A constellation of positive QuantiFERON-TB Gold In-Tube test, elevated ascitic adenosine deaminase and dramatic symptomatic and radiographic response to empiric anti-tuberculous therapy confirmed the diagnosis of peritoneal tuberculosis. This paper will review the approach to the diagnosis of peritoneal tuberculosis.
Keywords: TB and other respiratory infections; cirrhosis; global health; infection (gastroenterology); infections.
© BMJ Publishing Group Limited 2020. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Sophia De Saram JSF. Gastrointestinal and Peritoneal Tuberculosis : ASaH E, Extrapulmonary tuberculosis. 1 ed Springer International Publishing, 2019: 25–42.
-
- Sharma MP, Bhatia V. Abdominal tuberculosis. Indian J Med Res 2004;120:305–15. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials