

Improving cancer immunotherapy using nanomedicines: progress, opportunities and challenges
- PMID: 32034288
- PMCID: PMC8272676
- DOI: 10.1038/s41571-019-0308-z
Improving cancer immunotherapy using nanomedicines: progress, opportunities and challenges
Abstract
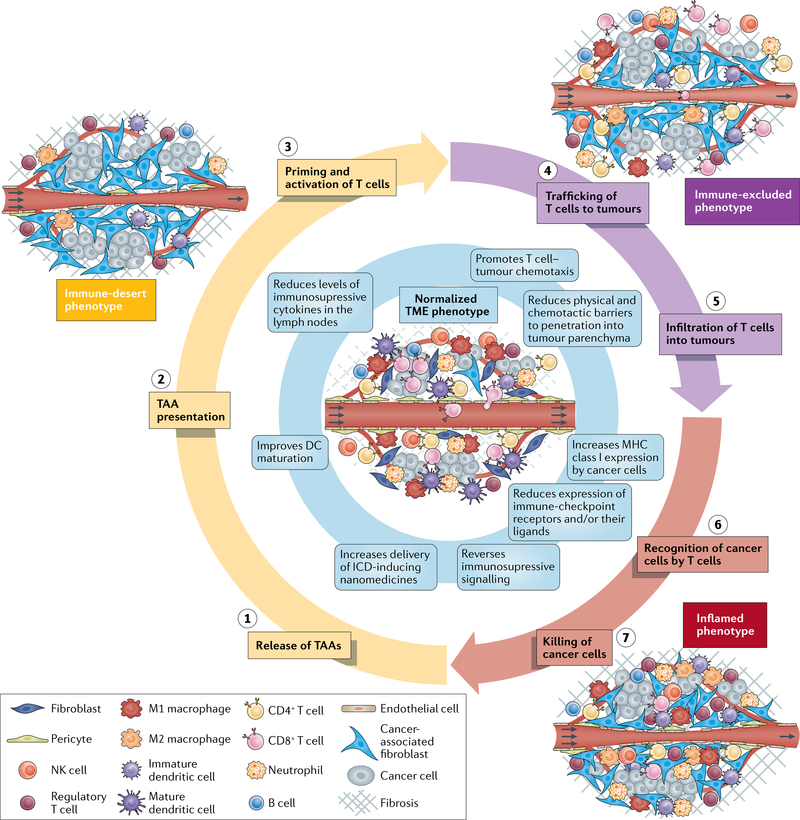
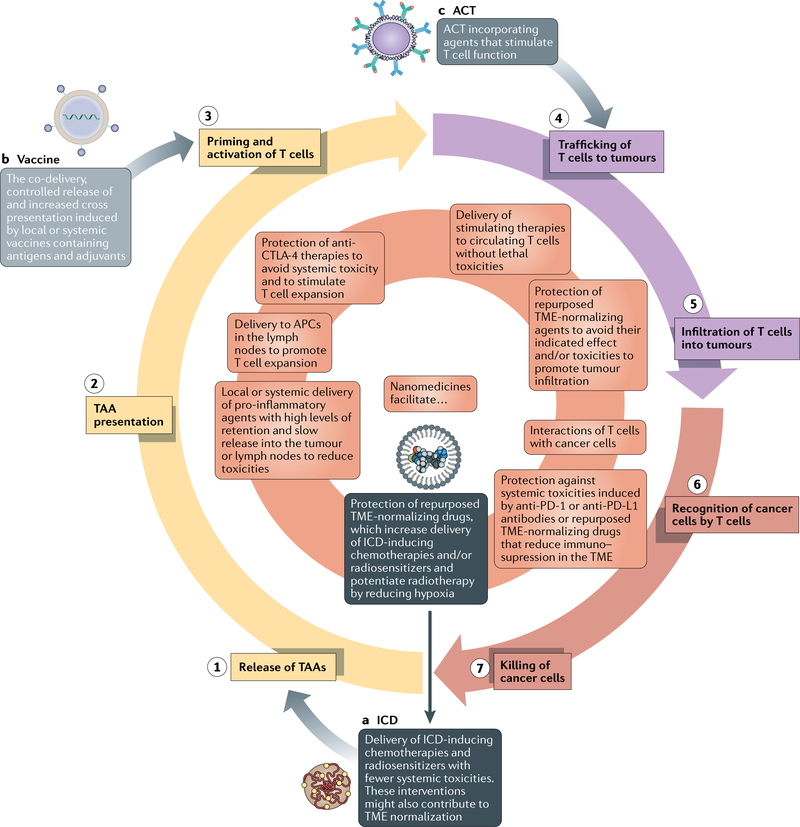
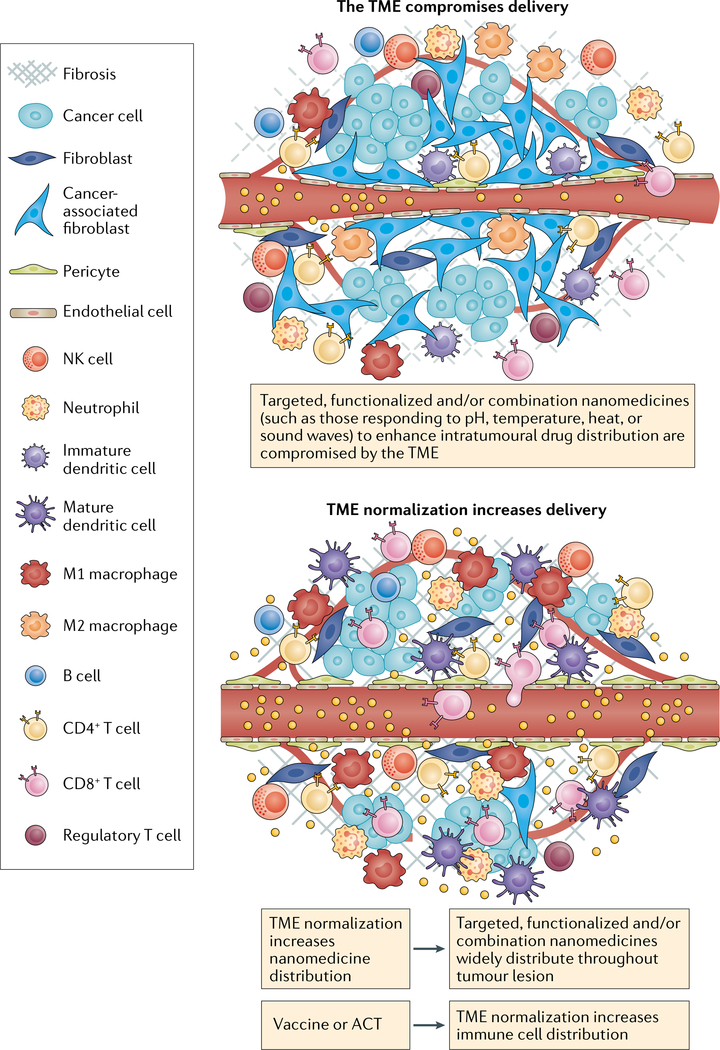
Multiple nanotherapeutics have been approved for patients with cancer, but their effects on survival have been modest and, in some examples, less than those of other approved therapies. At the same time, the clinical successes achieved with immunotherapy have revolutionized the treatment of multiple advanced-stage malignancies. However, the majority of patients do not benefit from the currently available immunotherapies and many develop immune-related adverse events. By contrast, nanomedicines can reduce - but do not eliminate - the risk of certain life-threatening toxicities. Thus, the combination of these therapeutic classes is of intense research interest. The tumour microenvironment (TME) is a major cause of the failure of both nanomedicines and immunotherapies that not only limits delivery, but also can compromise efficacy, even when agents accumulate in the TME. Coincidentally, the same TME features that impair nanomedicine delivery can also cause immunosuppression. In this Perspective, we describe TME normalization strategies that have the potential to simultaneously promote the delivery of nanomedicines and reduce immunosuppression in the TME. Then, we discuss the potential of a combined nanomedicine-based TME normalization and immunotherapeutic strategy designed to overcome each step of the cancer-immunity cycle and propose a broadly applicable 'minimal combination' of therapies designed to increase the number of patients with cancer who are able to benefit from immunotherapy.
Conflict of interest statement
Competing interests
J.D.M. became a full-time employee of NanoCarrier during the preparation of this manuscript. R.K.J. has received honoraria from Amgen, has acted as a consultant for Chugai, Merck, Ophthotech, Pfizer, SPARC, SynDevRx and XTuit, owns equity in Enlight, Ophthotech and SynDevRx and serves on the Boards of Trustees of Tekla Healthcare Investors, Tekla Life Sciences Investors, Tekla Healthcare Opportunities Fund and Tekla World Healthcare Fund. H.C. and T.S. declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
