

ESC Working Group on Coronary Pathophysiology and Microcirculation position paper on 'coronary microvascular dysfunction in cardiovascular disease'
- PMID: 32034397
- PMCID: PMC7825482
- DOI: 10.1093/cvr/cvaa003
ESC Working Group on Coronary Pathophysiology and Microcirculation position paper on 'coronary microvascular dysfunction in cardiovascular disease'
Abstract
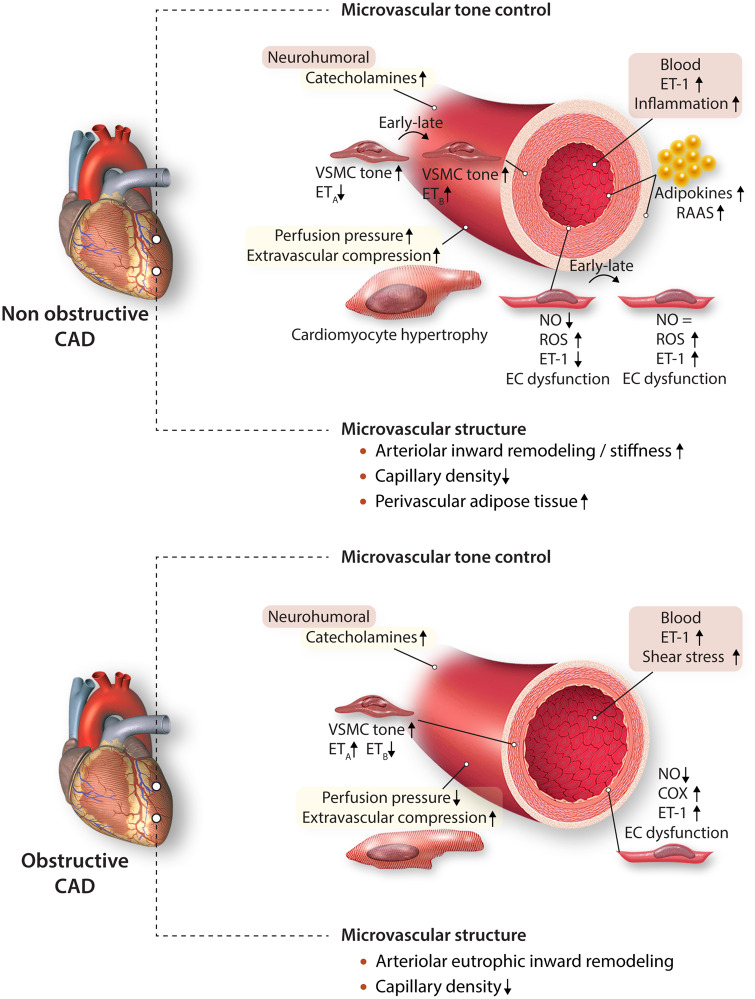
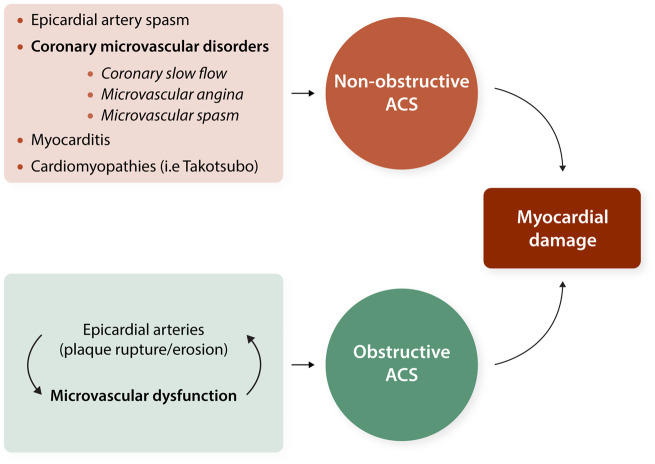
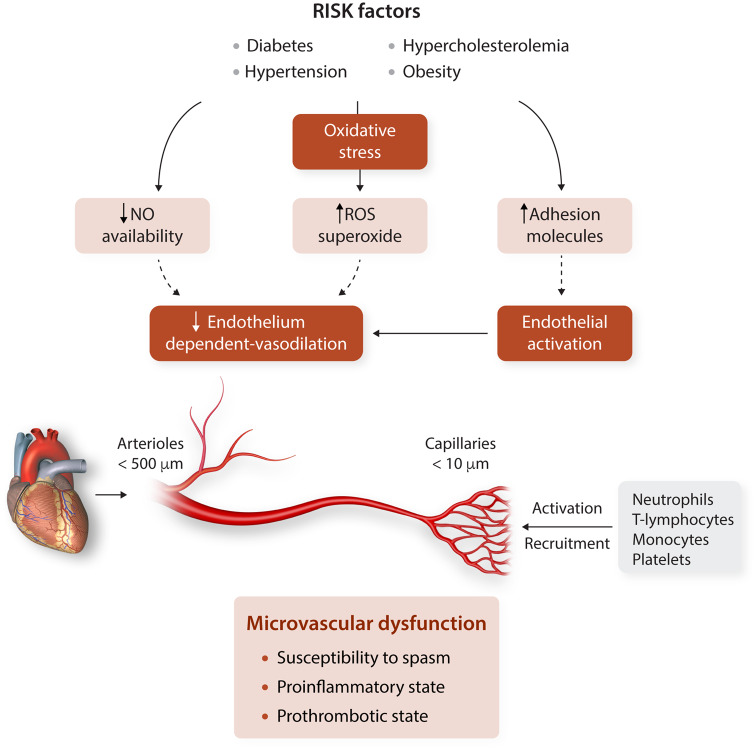
Although myocardial ischaemia usually manifests as a consequence of atherosclerosis-dependent obstructive epicardial coronary artery disease, a significant percentage of patients suffer ischaemic events in the absence of epicardial coronary artery obstruction. Experimental and clinical evidence highlight the abnormalities of the coronary microcirculation as a main cause of myocardial ischaemia in patients with 'normal or near normal' coronary arteries on angiography. Coronary microvascular disturbances have been associated with early stages of atherosclerosis even prior to any angiographic evidence of epicardial coronary stenosis, as well as to other cardiac pathologies such as myocardial hypertrophy and heart failure. The main objectives of the manuscript are (i) to provide updated evidence in our current understanding of the pathophysiological consequences of microvascular dysfunction in the heart; (ii) to report on the current knowledge on the relevance of cardiovascular risk factors and comorbid conditions for microcirculatory dysfunction; and (iii) to evidence the relevance of the clinical consequences of microvascular dysfunction. Highlighting the clinical importance of coronary microvascular dysfunction will open the field for research and the development of novel strategies for intervention will encourage early detection of subclinical disease and will help in the stratification of cardiovascular risk in agreement with the new concept of precision medicine.
Keywords: Coronary microcirculation; Ischaemic heart disease; Microvessels; Molecular and cellular targets; Risk factors.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.
Figures

References
-
- Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, Prescott E, Storey RF, Deaton C, Cuisset T, Agewall S, Dickstein K, Edvardsen T, Escaned J, Gersh BJ, Svitil P, Gilard M, Hasdai D, Hatala R, Mahfoud F, Masip J, Muneretto C, Valgimigli M, Achenbach S, Bax JJ, Neumann F-J, Sechtem U, Banning AP, Bonaros N, Bueno H, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J 2020;41:407-477. - PubMed
-
- Ong P, Camici PG, Beltrame JF, Crea F, Shimokawa H, Sechtem U, Kaski JC, Bairey Merz CN; Coronary Vasomotion Disorders International Study Group (COVADIS). International standardization of diagnostic criteria for microvascular angina. Int J Cardiol 2018;250:16–20. - PubMed
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, Caforio ALP, Crea F, Goudevenos JA, Halvorsen S, Hindricks G, Kastrati A, Lenzen MJ, Prescott E, Roffi M, Valgimigli M, Varenhorst C, Vranckx P, Widimský P; ESC Scientific Document Group. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2018;39:119–177. - PubMed
-
- Agewall S, Beltrame JF, Reynolds HR, Niessner A, Rosano G, Caforio ALP, De Caterina R, Zimarino M, Roffi M, Kjeldsen K, Atar D, Kaski JC, Sechtem U, Tornvall P; WG on Cardiovascular Pharmacotherapy. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J 2017;38:143–153. - PubMed
