

Prediction of survival in patients with IDH-wildtype astrocytic gliomas using dynamic O-(2-[18F]-fluoroethyl)-L-tyrosine PET
- PMID: 32034446
- PMCID: PMC7188701
- DOI: 10.1007/s00259-020-04695-0
Prediction of survival in patients with IDH-wildtype astrocytic gliomas using dynamic O-(2-[18F]-fluoroethyl)-L-tyrosine PET
Abstract
Purpose: Integrated histomolecular diagnostics of gliomas according to the World Health Organization (WHO) classification of 2016 has refined diagnostic accuracy and prediction of prognosis. This study aimed at exploring the prognostic value of dynamic O-(2-[18F]-fluoroethyl)-L-tyrosine (FET) PET in newly diagnosed, histomolecularly classified astrocytic gliomas of WHO grades III or IV.
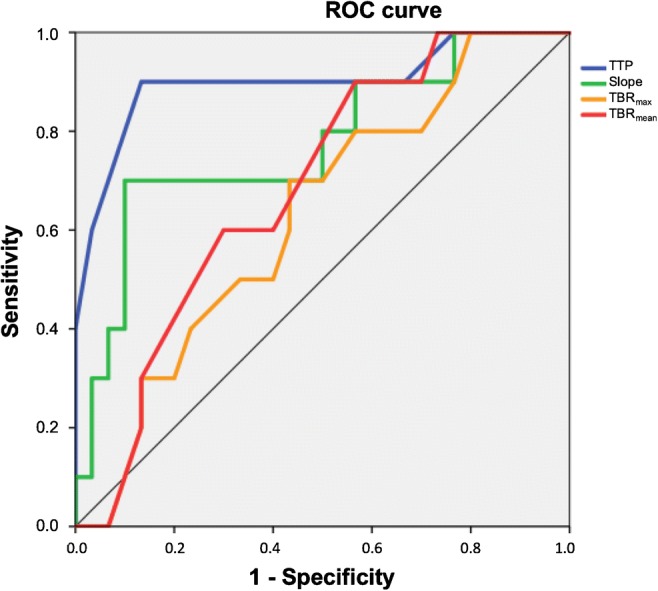
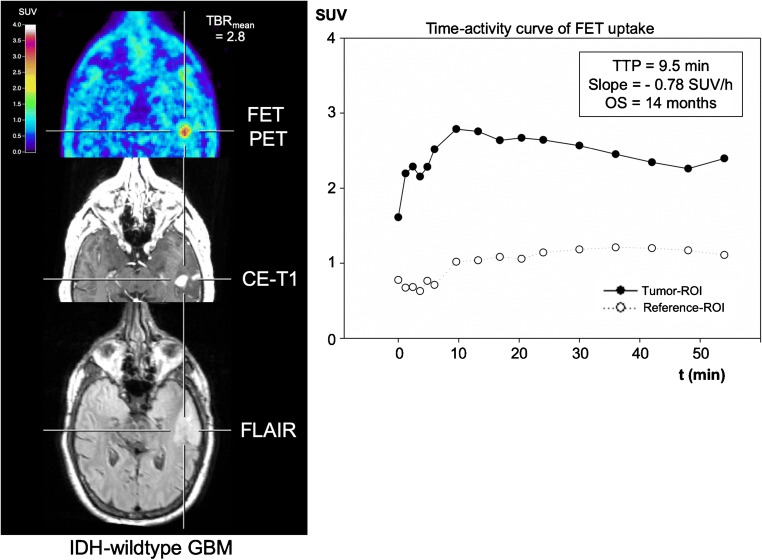
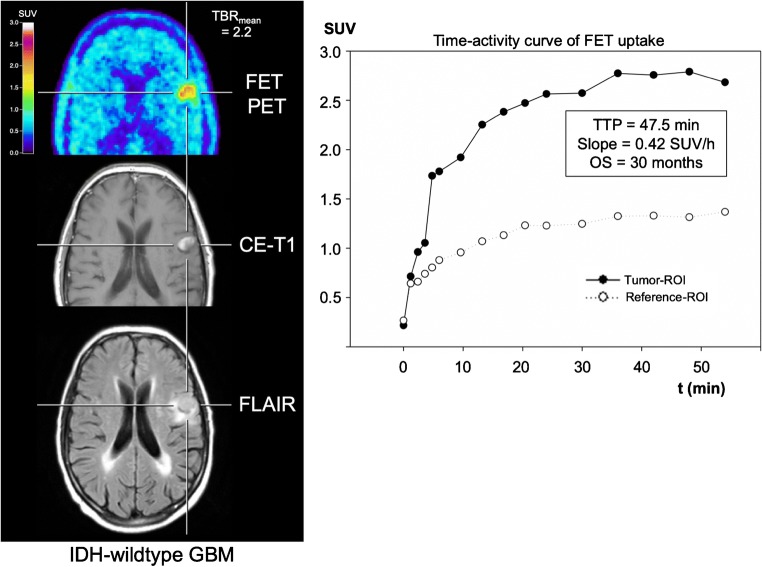
Methods: Before initiation of treatment, dynamic FET PET imaging was performed in patients with newly diagnosed glioblastoma (GBM) and anaplastic astrocytoma (AA). Static FET PET parameters such as maximum and mean tumour/brain ratios (TBRmax/mean), the metabolic tumour volume (MTV) as well as the dynamic FET PET parameters time-to-peak (TTP) and slope, were obtained. The predictive ability of FET PET parameters was evaluated concerning the progression-free and overall survival (PFS, OS). Using ROC analyses, threshold values for FET PET parameters were obtained. Subsequently, univariate Kaplan-Meier and multivariate Cox regression survival analyses were performed to assess the predictive power of these parameters for survival.
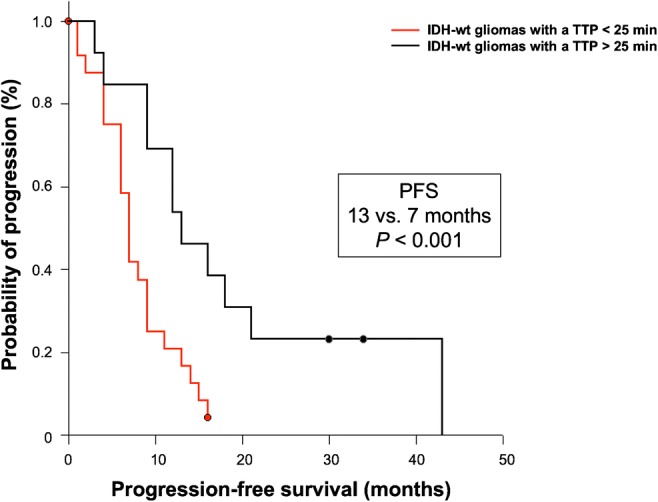
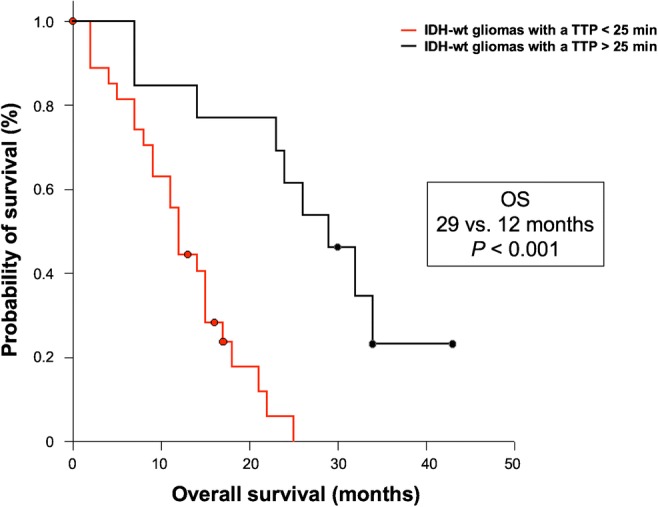
Results: Sixty patients (45 GBM and 15 AA patients) of two university centres were retrospectively identified. Patients with isocitrate dehydrogenase (IDH)-mutant or O6-methylguanine-DNA-methyltransferase (MGMT) promoter-methylated tumours had a significantly longer PFS and OS (both P < 0.001). Furthermore, ROC analysis of IDH-wildtype glioma patients (n = 45) revealed that a TTP > 25 min (AUC, 0.90; sensitivity, 90%; specificity, 87%; P < 0.001) was highly prognostic for longer PFS (13 vs. 7 months; P = 0.005) and OS (29 vs. 12 months; P < 0.001). In contrast, at a lower level of significance, TBRmax, TBRmean, and MTV were only prognostic for longer OS (P = 0.004, P = 0.038, and P = 0.048, respectively). Besides complete resection and a methylated MGMT promoter, TTP remained significant in multivariate survival analysis (all P ≤ 0.02), indicating an independent predictor for OS.
Conclusions: Our data suggest that dynamic FET PET allows the identification of patients with longer OS among patients with newly diagnosed IDH-wildtype GBM and AA.
Keywords: FET PET; High-grade glioma; IDH mutation; MGMT promoter methylation; Overall survival.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
