

Diagnostic Value of Electroencephalography with Ten Electrodes in Critically Ill Patients
- PMID: 32034656
- PMCID: PMC7416437
- DOI: 10.1007/s12028-019-00911-4
Diagnostic Value of Electroencephalography with Ten Electrodes in Critically Ill Patients
Abstract
Background: In critical care settings, electroencephalography (EEG) with reduced number of electrodes (reduced montage EEG, rm-EEG) might be a timely alternative to the conventional full montage EEG (fm-EEG). However, past studies have reported variable accuracies for detecting seizures using rm-EEG. We hypothesized that the past studies did not distinguish between differences in sensitivity from differences in classification of EEG patterns by different readers. The goal of the present study was to revisit the diagnostic value of rm-EEG when confounding issues are accounted for.
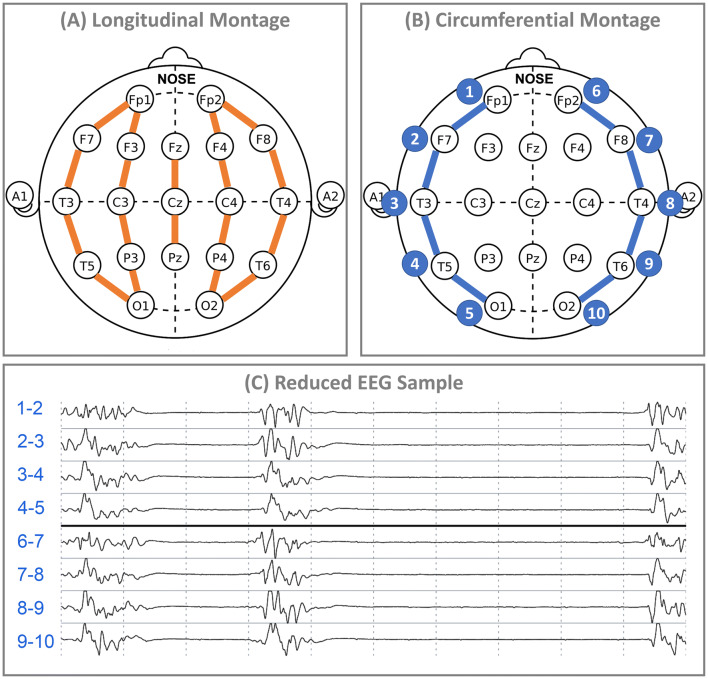
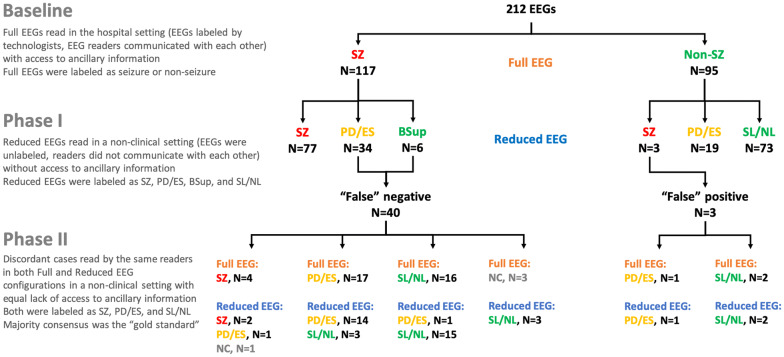
Methods: We retrospectively collected 212 adult EEGs recorded at Massachusetts General Hospital and reviewed by two epileptologists with access to clinical, trending, and video information. In Phase I of the study, we re-configured the first 4 h of the EEGs in lateral circumferential montage with ten electrodes and asked new readers to interpret the EEGs without access to any other ancillary information. We compared their rating to the reading of hospital clinicians with access to ancillary information. In Phase II, we measured the accuracy of the same raters reading representative samples of the discordant EEGs in full and reduced configurations presented randomly by comparing their performance to majority consensus as the gold standard.
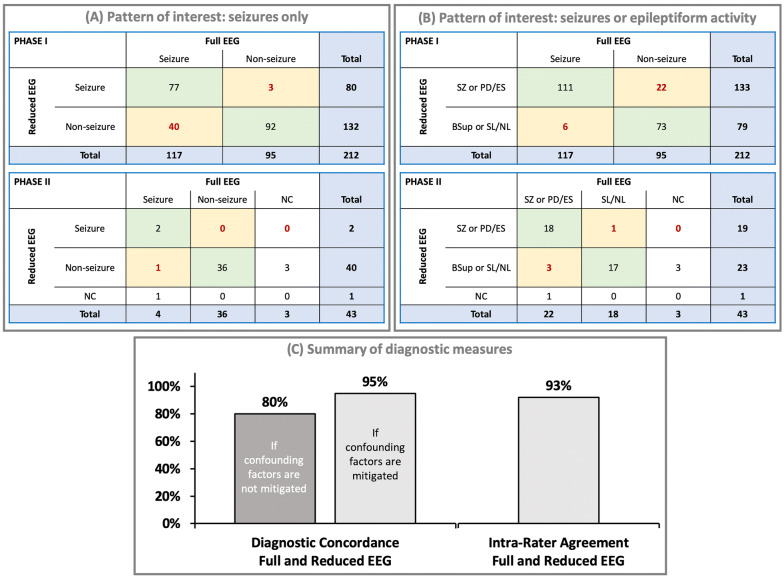
Results: Of the 95 EEGs without seizures in the selected fm-EEG, readers of rm-EEG identified 92 cases (97%) as having no seizure activity. Of 117 EEGs with "seizures" identified in the selected fm-EEG, none of the cases was labeled as normal on rm-EEG. Readers of rm-EEG reported pathological activity in 100% of cases, but labeled them as seizures (N = 77), rhythmic or periodic patterns (N = 24), epileptiform spikes (N = 7), or burst suppression (N = 6). When the same raters read representative epochs of the discordant EEG cases (N = 43) in both fm-EEG and rm-EEG configurations, we found high concordance (95%) and intra-rater agreement (93%) between fm-EEG and rm-EEG diagnoses.
Conclusions: Reduced EEG with ten electrodes in circumferential configuration preserves key features of the traditional EEG system. Discrepancies between rm-EEG and fm-EEG as reported in some of the past studies can be in part due to methodological factors such as choice of gold standard diagnosis, asymmetric access to ancillary clinical information, and inter-rater variability rather than detection failure of rm-EEG as a result of electrode reduction per se.
Keywords: Abbreviated EEG; Continuous EEG monitoring; Electroencephalography (EEG); Neuroemergencies; Non-convulsive status epilepticus; Seizure prediction.
Conflict of interest statement
Dr. Westover reports no conflict of interest. Dr. Gururangan has received compensation from Ceribell to work on data compilation and statistical analysis. Drs. Markert, Blond, Lai, Benard, and Bickel were all clinical epileptologists outside MGH at the time of the study who were compensated for their time to review EEGs, but otherwise report no relevant conflicts of interest. Dr. Hirsch serves as scientific and clinical advisor to Ceribell. Dr. Parvizi is one of the inventors of Rapid Response EEG system. He is also co-founder of Ceribell, which is a commercial company based in Silicon Valley, CA developing the Rapid Response EEG system for clinical use. Dr. Parvizi’s contribution to this publication was not part of his Stanford University duties or responsibilities.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
