

Efficacy gap between phase II and subsequent phase III studies in oncology
- PMID: 32034790
- PMCID: PMC7318994
- DOI: 10.1111/bcp.14237
Efficacy gap between phase II and subsequent phase III studies in oncology
Abstract
Aims: There is a trend for more flexibility in timing of evidence generation in relation to marketing authorization, including the option to complete phase III trials after authorization or not at all. This paper investigated the relation between phase II and III clinical trial efficacy in oncology.
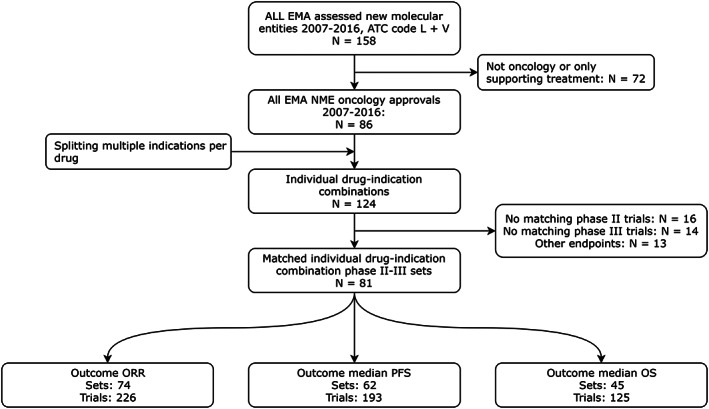
Methods: All oncology drugs approved by the European Medicines Agency (2007-2016) were included. Phase II and phase III trials were matched based on indication and treatment and patient characteristics. Reported objective response rates (ORR), median progression-free survival (PFS) and median overall survival (OS) were analysed through weighted mixed-effects regression with previous treatment, treatment regimen, blinding, randomization, marketing authorization type and cancer type as covariates.
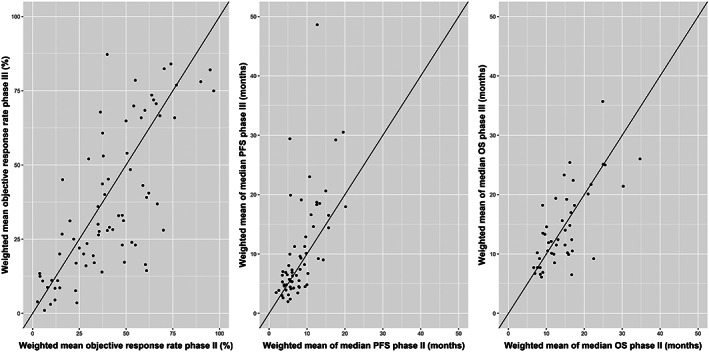
Results: A total of 81 phase II-III matches were identified including 252 trials. Mean (standard deviation) weighted difference (phase III minus II) was -4.2% (17.4) for ORR, 2.1 (6.7) months for PFS and -0.3 (5.1) months for OS, indicating very small average differences between phases. Differences varied substantially between individual indications: from -46.6% to 47.3% for ORR, from -5.3 to 35.9 months for PFS and from -13.3 to 10.8 months for OS. All covariates except blinding were associated with differences in effect sizes for at least 1 outcome.
Conclusions: The lack of marked average differences between phases may encourage decision-makers to regard the quality of design and total body of evidence instead of differentiating between phases of clinical development. The large variability emphasizes that replication of study findings remains essential to confirm efficacy of oncology drugs and discern variables associated with demonstrated effects.
Keywords: clinical trials; conditional marketing authorization; efficacy; oncology; phase; regulation.
© 2020 The Authors. British Journal of Clinical Pharmacology published by John Wiley & Sons Ltd on behalf of British Pharmacological Society.
Conflict of interest statement
R.A.V. reports funding from the Governmental Dutch National Health Care Institute for the submitted work. All other authors declare no support from any organization for the submitted work; A.M.H. reports unrestricted grants from GlaxoSmithKline, outside the submitted work. H.G.M.L. reports that he is past‐chairman of the Dutch Medicines Evaluation Board and past‐member of the EMA Committee for Medicinal Products for Human Use. He also reports that he is a member of the Lygature Leadership Team. The other authors declare no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- International Council for Harmonisation (ICH) . E8 General Considerations for Clinical Trials. Switserland. 1997. [Internet]. [cited 2018 Sep 7]. Available from: http://www.ich.org/products/guidelines/efficacy/efficacy-single/article/...
-
- European Medicines Agency . CPMP. E8 (CPMP/ICH/291/95) General Considerations for Clinical Trials. London. 1997. [Internet]. [cited 2018. Sep 7]. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/regulation/general/gen...
-
- Morant AV, Vestergaard HT. European marketing authorizations granted based on a single pivotal clinical trial: the rule or the exception? Clinical Pharmacology & Therapeutics. 2018;104(1):169‐177. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
