

Prophylactic biological mesh reinforcement versus standard closure of stoma site (ROCSS): a multicentre, randomised controlled trial
- PMID: 32035551
- PMCID: PMC7016509
- DOI: 10.1016/S0140-6736(19)32637-6
Prophylactic biological mesh reinforcement versus standard closure of stoma site (ROCSS): a multicentre, randomised controlled trial
Abstract
Background: Closure of an abdominal stoma, a common elective operation, is associated with frequent complications; one of the commonest and impactful is incisional hernia formation. We aimed to investigate whether biological mesh (collagen tissue matrix) can safely reduce the incidence of incisional hernias at the stoma closure site.
Methods: In this randomised controlled trial (ROCSS) done in 37 hospitals across three European countries (35 UK, one Denmark, one Netherlands), patients aged 18 years or older undergoing elective ileostomy or colostomy closure were randomly assigned using a computer-based algorithm in a 1:1 ratio to either biological mesh reinforcement or closure with sutures alone (control). Training in the novel technique was standardised across hospitals. Patients and outcome assessors were masked to treatment allocation. The primary outcome measure was occurrence of clinically detectable hernia 2 years after randomisation (intention to treat). A sample size of 790 patients was required to identify a 40% reduction (25% to 15%), with 90% power (15% drop-out rate). This study is registered with ClinicalTrials.gov, NCT02238964.
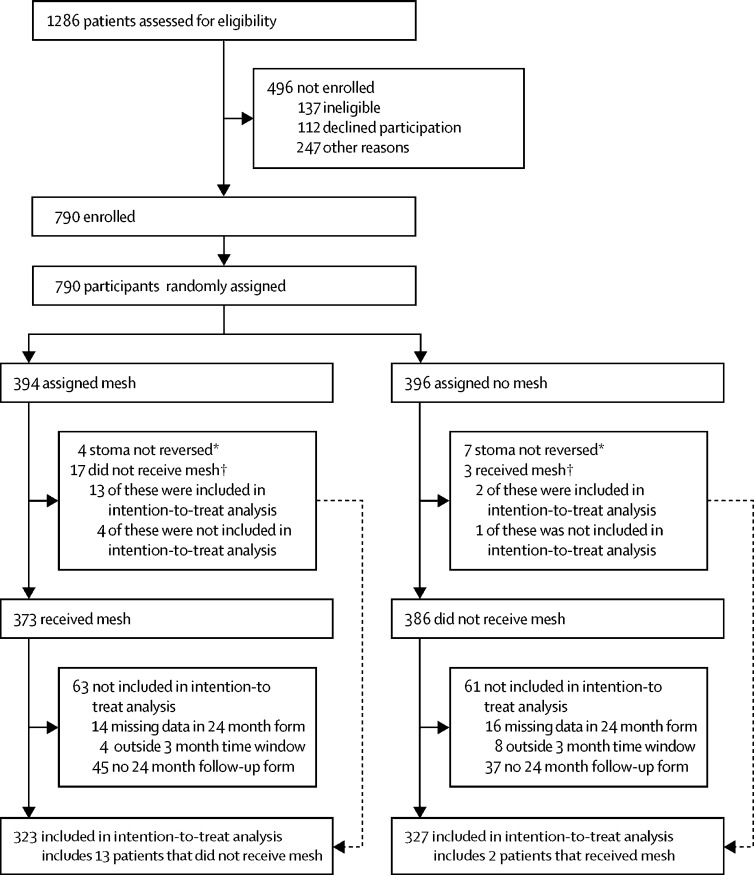
Findings: Between Nov 28, 2012, and Nov 11, 2015, of 1286 screened patients, 790 were randomly assigned. 394 (50%) patients were randomly assigned to mesh closure and 396 (50%) to standard closure. In the mesh group, 373 (95%) of 394 patients successfully received mesh and in the control group, three patients received mesh. The clinically detectable hernia rate, the primary outcome, at 2 years was 12% (39 of 323) in the mesh group and 20% (64 of 327) in the control group (adjusted relative risk [RR] 0·62, 95% CI 0·43-0·90; p=0·012). In 455 patients for whom 1 year postoperative CT scans were available, there was a lower radiologically defined hernia rate in mesh versus control groups (20 [9%] of 229 vs 47 [21%] of 226, adjusted RR 0·42, 95% CI 0·26-0·69; p<0·001). There was also a reduction in symptomatic hernia (16%, 52 of 329 vs 19%, 64 of 331; adjusted relative risk 0·83, 0·60-1·16; p=0·29) and surgical reintervention (12%, 42 of 344 vs 16%, 54 of 346: adjusted relative risk 0·78, 0·54-1·13; p=0·19) at 2 years, but this result did not reach statistical significance. No significant differences were seen in wound infection rate, seroma rate, quality of life, pain scores, or serious adverse events.
Interpretation: Reinforcement of the abdominal wall with a biological mesh at the time of stoma closure reduced clinically detectable incisional hernia within 24 months of surgery and with an acceptable safety profile. The results of this study support the use of biological mesh in stoma closure site reinforcement to reduce the early formation of incisional hernias.
Funding: National Institute for Health Research Research for Patient Benefit and Allergan.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Stoma closure reinforcement with biological mesh and incisional hernia.Lancet. 2020 Feb 8;395(10222):393-395. doi: 10.1016/S0140-6736(19)32958-7. Lancet. 2020. PMID: 32035534 No abstract available.
References
-
- NHS Digital Hospital Episode Statistics. 2019. https://digital.nhs.uk/data-and-information/data-tools-and-services/data...
-
- Doussot A, Abo-Alhassan F, Derbal S. Indications and outcomes of a cross-linked porcine dermal collagen mesh (permacol) for complex abdominal wall reconstruction: a multicenter audit. World J Surg. 2019;43:791–797. - PubMed
-
- Bhangu A, Nepogodiev D, Futaba K. Systematic review and meta-analysis of the incidence of incisional hernia at the site of stoma closure. World J Surg. 2012;36:973–983. - PubMed
-
- Bhangu A, Fletcher L, Kingdon S, Smith E, Nepogodiev D, Janjua U. A clinical and radiological assessment of incisional hernias following closure of temporary stomas. Surgeon. 2012;10:321–325. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
