Role of ultrasound in the evaluation of first-trimester pregnancies in the acute setting
- PMID: 32036643
- PMCID: PMC7065984
- DOI: 10.14366/usg.19043
Role of ultrasound in the evaluation of first-trimester pregnancies in the acute setting
Abstract
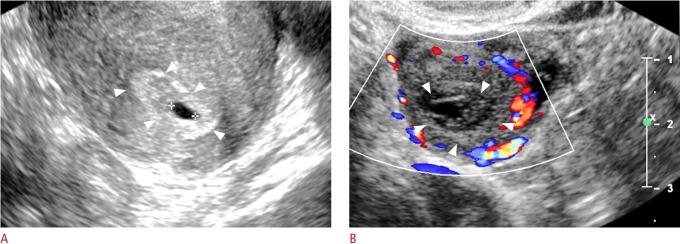
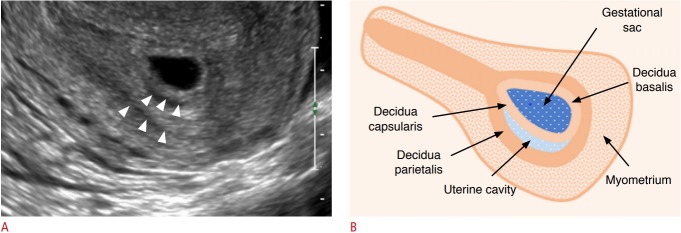
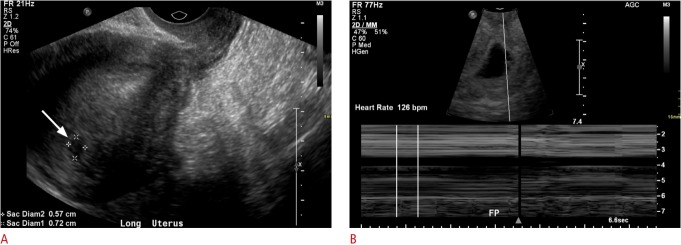
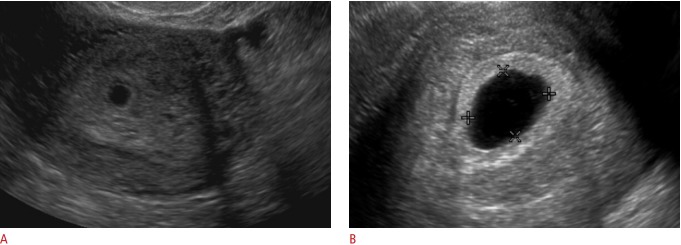
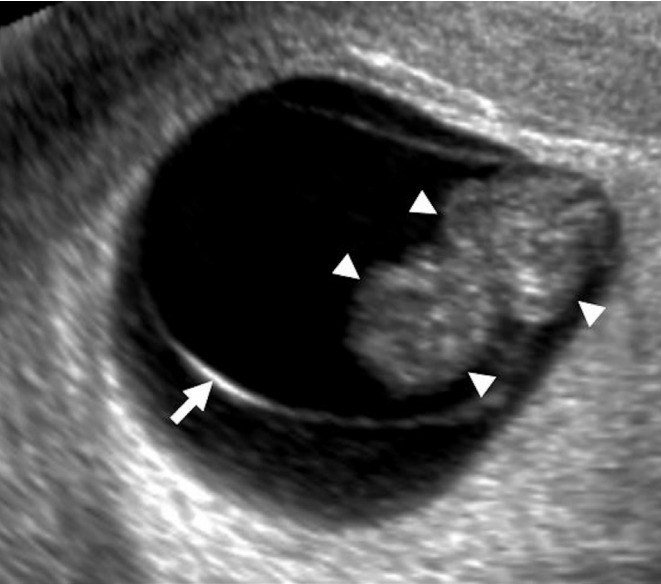
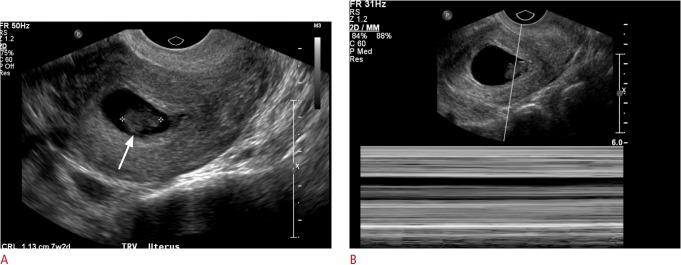
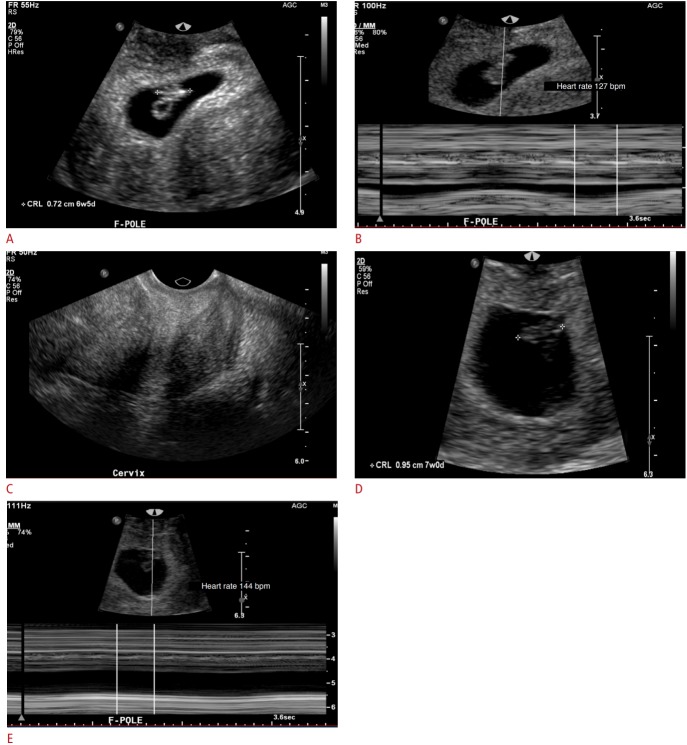
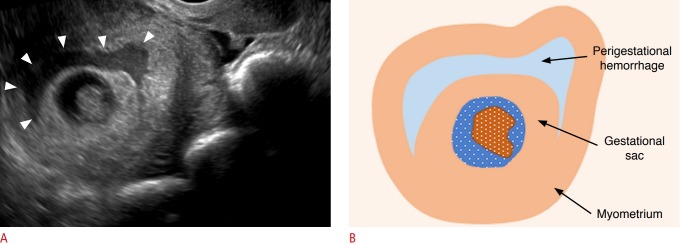
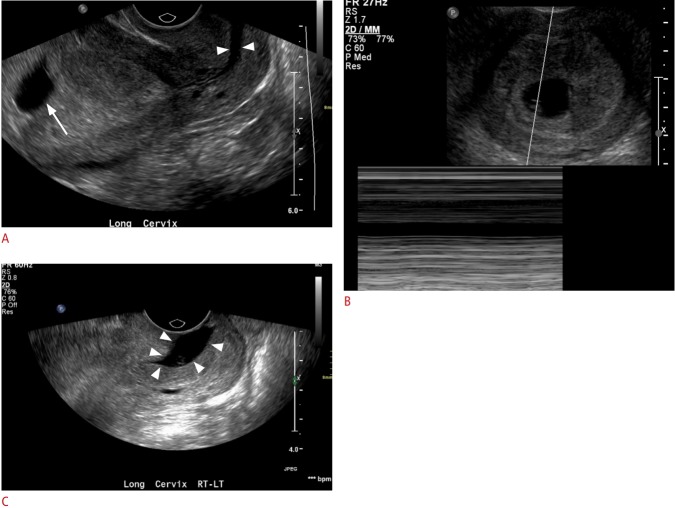
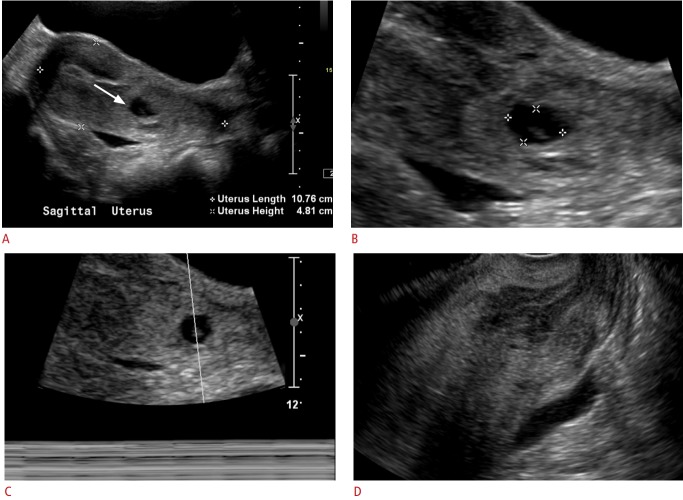
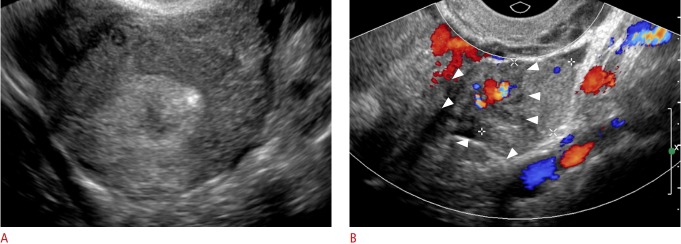
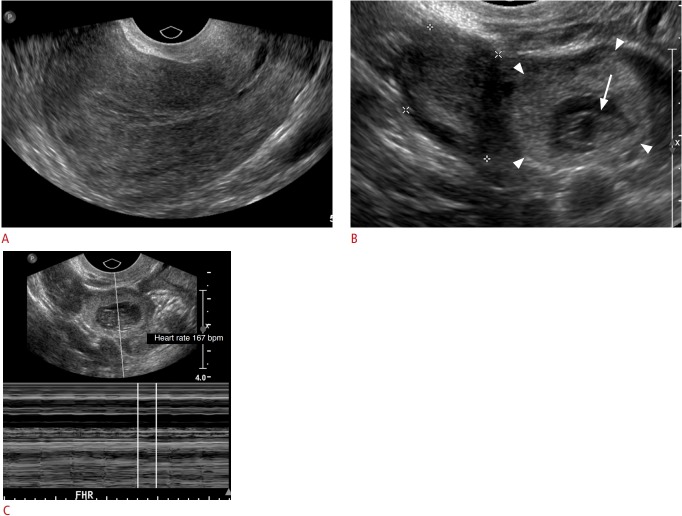
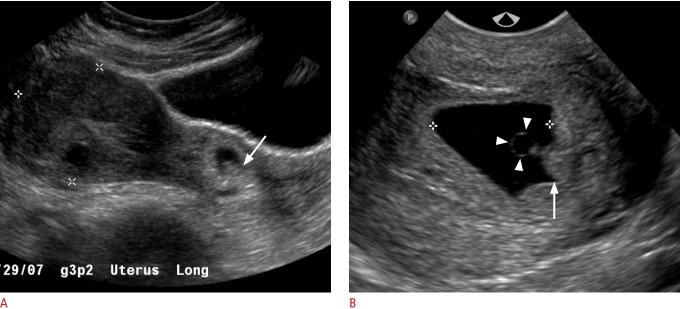
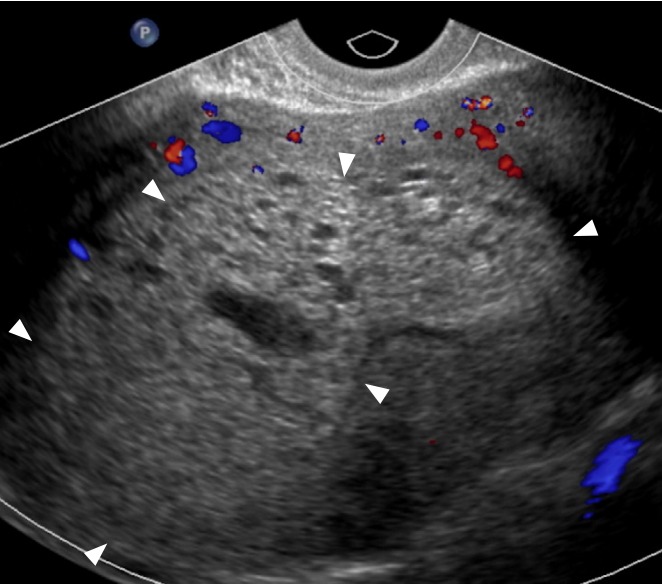
In patients presenting for an evaluation of pregnancy in the first trimester, transvaginal ultrasound is the modality of choice for establishing the presence of an intrauterine pregnancy; evaluating pregnancy viability, gestational age, and multiplicity; detecting pregnancy-related complications; and diagnosing ectopic pregnancy. In this pictorial review article, the sonographic appearance of a normal intrauterine gestation and the most common complications of pregnancy in the first trimester in the acute setting are discussed.
Keywords: Abnormal gestation; Abortion; Ectopic pregnancy; Transvaginal ultrasound; Viability.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures

References
-
- AIUM-ACR-ACOG-SMFM-SRU practice parameter for the performance of standard diagnostic obstetric ultrasound examinations. J Ultrasound Med. 2018;37:E13–E24. - PubMed
-
- Doubilet PM. Ultrasound evaluation of the first trimester. Radiol Clin North Am. 2014;52:1191–1199. - PubMed
-
- Nyberg DA, Mack LA, Laing FC, Patten RM. Distinguishing normal from abnormal gestational sac growth in early pregnancy. J Ultrasound Med. 1987;6:23–27. - PubMed
-
- Doubilet PM, Benson CB. First, do no harm... To early pregnancies. J Ultrasound Med. 2010;29:685–689. - PubMed
-
- Doubilet PM, Benson CB, Bourne T, Blaivas M, Society of Radiologists in Ultrasound Multispecialty Panel on Early First Trimester Diagnosis of Miscarriage and Exclusion of a Viable Intrauterine Pregnancy. Barnhart KT, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med. 2013;369:1443–1451. - PubMed
LinkOut - more resources
Full Text Sources