

Comparative study of the Ambu® AuraOnce™ laryngeal mask and endotracheal intubation in anesthesia airway management during neurosurgery
- PMID: 32036718
- PMCID: PMC7111043
- DOI: 10.1177/0300060520902606
Comparative study of the Ambu® AuraOnce™ laryngeal mask and endotracheal intubation in anesthesia airway management during neurosurgery
Abstract
Objective: To investigate the feasibility and efficacy of the Ambu® AuraOnce™ laryngeal mask (LMA) compared with endotracheal intubation (ETI) during supratentorial tumor resection in the right lateral decubitus position.
Methods: This was a randomized controlled trial of LMA compared with ETI in patients who were scheduled to undergo supratentorial tumor resection in the right lateral decubitus position. The patients were randomized to the LMA (n = 40) and ETI groups (n = 40). The hemodynamic parameters (primary outcome) and mechanical ventilation parameters, anesthetic dose, and complications as well as quality of anesthesia recovery (secondary outcomes) were compared.
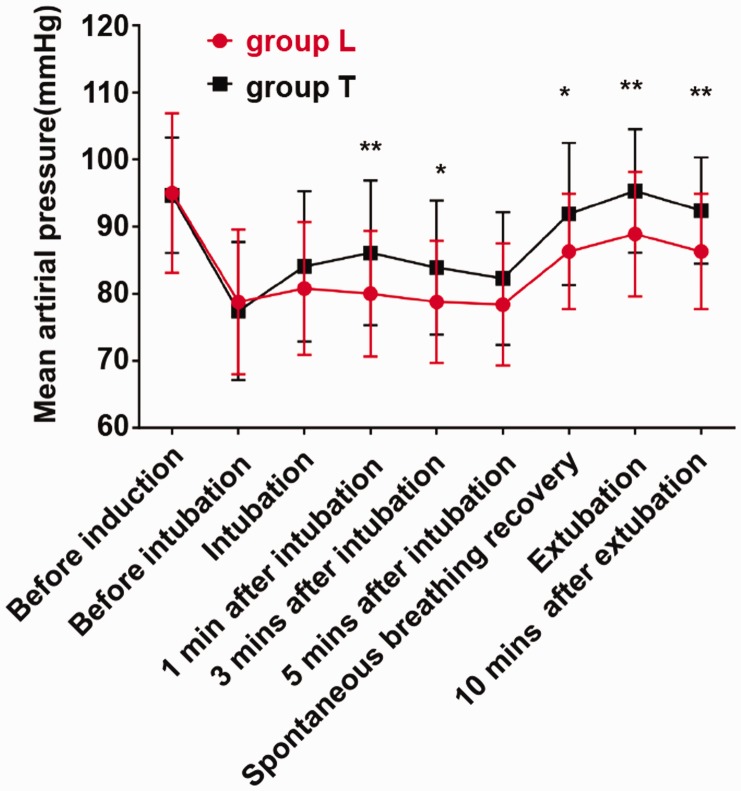
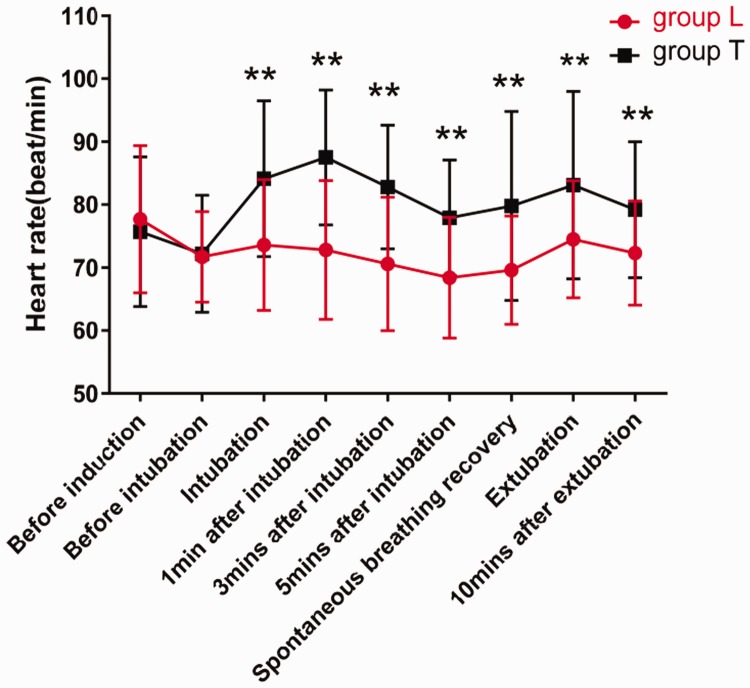
Results: Patients in the LMA group exhibited lower mean arterial pressure (MAP) and heart rate (HR) compared with ETI. Nine and two patients received esmolol during intubation and extubation, respectively. The airway pressure (AP) in the LMA group was higher compared with the ETI group 60 minutes after the start of surgery. Compared with the ETI group, the sufentanil dose was lower by 24% and the anesthesia recovery rate was better in the LMA group.
Conclusions: LMA can improve hemodynamic stability in patients undergoing supratentorial tumor resection in the right lateral decubitus position. If there is a clinical need and no contraindication, LMA could replace ETI.
Keywords: Laryngeal mask; airway management; comparative study; endotracheal intubation; hemodynamic stability; neurosurgical anesthesia; supratentorial tumor resection.
Figures
Similar articles
-
Influence of laryngeal mask airway (LMA) insertion anesthesia on cognitive function after microsurgery in pediatric neurosurgery.Eur Rev Med Pharmacol Sci. 2017 Oct;21(4 Suppl):37-42. Eur Rev Med Pharmacol Sci. 2017. PMID: 29165767 Clinical Trial.
-
Endotracheal intubation, but not laryngeal mask airway insertion, produces reversible bronchoconstriction.Anesthesiology. 1999 Feb;90(2):391-4. doi: 10.1097/00000542-199902000-00010. Anesthesiology. 1999. PMID: 9952142 Clinical Trial.
-
A comparison of blind intubation with the intubating laryngeal mask FASTRACH™ and the intubating laryngeal mask Ambu Aura-i™ a prospective randomised clinical trial.BMC Anesthesiol. 2019 Mar 30;19(1):44. doi: 10.1186/s12871-019-0718-6. BMC Anesthesiol. 2019. PMID: 30927922 Free PMC article. Clinical Trial.
-
[Airway equipment and its maintenance for a non difficult adult airway management (endotracheal intubation and its alternative: face mask, laryngeal mask airway, laryngeal tube)].Ann Fr Anesth Reanim. 2003 Aug;22 Suppl 1:28s-40s. doi: 10.1016/s0750-7658(03)00124-2. Ann Fr Anesth Reanim. 2003. PMID: 12943860 Review. French.
-
[Problems and complications in airway management by endotracheal intubation and laryngeal mask airway].Masui. 2006 Jan;55(1):44-50. Masui. 2006. PMID: 16440706 Review. Japanese.
Cited by
-
Multidisciplinary international expert consensus on perioperative airway management.Transl Lung Cancer Res. 2025 Apr 30;14(4):1042-1060. doi: 10.21037/tlcr-2025-273. Epub 2025 Apr 16. Transl Lung Cancer Res. 2025. PMID: 40386733 Free PMC article. Review.
-
Use of view-adjustable video laryngeal mask versus endotracheal intubation for airway management during anaesthesia for arthroscopic surgery: a randomized trial.Ann Med. 2025 Dec;57(1):2519683. doi: 10.1080/07853890.2025.2519683. Epub 2025 Jun 19. Ann Med. 2025. PMID: 40536491 Free PMC article. Clinical Trial.
-
Comparison of the Jcerity Endoscoper Airway with the LMA supreme for airway management in patients undergoing cerebral aneurysm embolization: a randomized controlled non-inferiority trial.BMC Anesthesiol. 2022 Apr 26;22(1):121. doi: 10.1186/s12871-022-01666-w. BMC Anesthesiol. 2022. PMID: 35473459 Free PMC article. Clinical Trial.
-
Influence of endotracheal tube and laryngeal mask airway for general anesthesia on perioperative adverse events in patients undergoing laparoscopic hysterectomy: A propensity score-matched analysis.J Res Med Sci. 2024 Feb 23;28:88. doi: 10.4103/jrms.jrms_384_22. eCollection 2023. J Res Med Sci. 2024. PMID: 38510782 Free PMC article.
-
Laryngeal mask airway versus endotracheal intubation as general anesthesia airway managements for atrial fibrillation catheter ablation: a comparative analysis based on propensity score matching.J Interv Card Electrophysiol. 2024 Sep;67(6):1377-1390. doi: 10.1007/s10840-024-01742-w. Epub 2024 Jan 16. J Interv Card Electrophysiol. 2024. PMID: 38225533
References
-
- Perello-Cerda L, Fabregas N, Lopez AMet al. ProSeal laryngeal mask airway attenuates systemic and cerebral hemodynamic response during awakening of neurosurgical patients: A randomized clinical trial. J Neurosurg Anesthesiol 2015; 27: 194–202. - PubMed
-
- Russo SG, Goetze B, Troche Set al. LMA-ProSeal for elective postoperative care on the intensive care unit: A prospective, randomized trial. Anesthesiology 2009; 111: 116–121. - PubMed
-
- Carron M, Veronese S, Gomiero Wet al. Hemodynamic and hormonal stress responses to endotracheal tube and ProSeal laryngeal mask airway for laparoscopic gastric banding. Anesthesiology 2012; 117: 309–320. - PubMed
-
- Wong AY, O’Regan AM, Irwin MG. Total intravenous anaesthesia with propofol and remifentanil for elective neurosurgical procedures: an audit of early postoperative complications. Eur J Anaesthesiol 2006; 23: 586–590. - PubMed
-
- Bruder N, Pellissier D, Grillot Pet al. Cerebral hyperemia during recovery from general anesthesia in neurosurgical patients. Anesth Analg 2002; 94: 650–654; table of contents. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
