

Combined lifestyle factors, incident cancer, and cancer mortality: a systematic review and meta-analysis of prospective cohort studies
- PMID: 32037402
- PMCID: PMC7109112
- DOI: 10.1038/s41416-020-0741-x
Combined lifestyle factors, incident cancer, and cancer mortality: a systematic review and meta-analysis of prospective cohort studies
Abstract
Background: Cancer poses a huge disease burden, which could be reduced by adopting healthy lifestyles mainly composed of healthy diet, body weight, physical activity, limited alcohol consumption, and avoidance of smoking. However, no systematic review has summarised the relations of combined lifestyle factors with cancer morbidity and mortality.
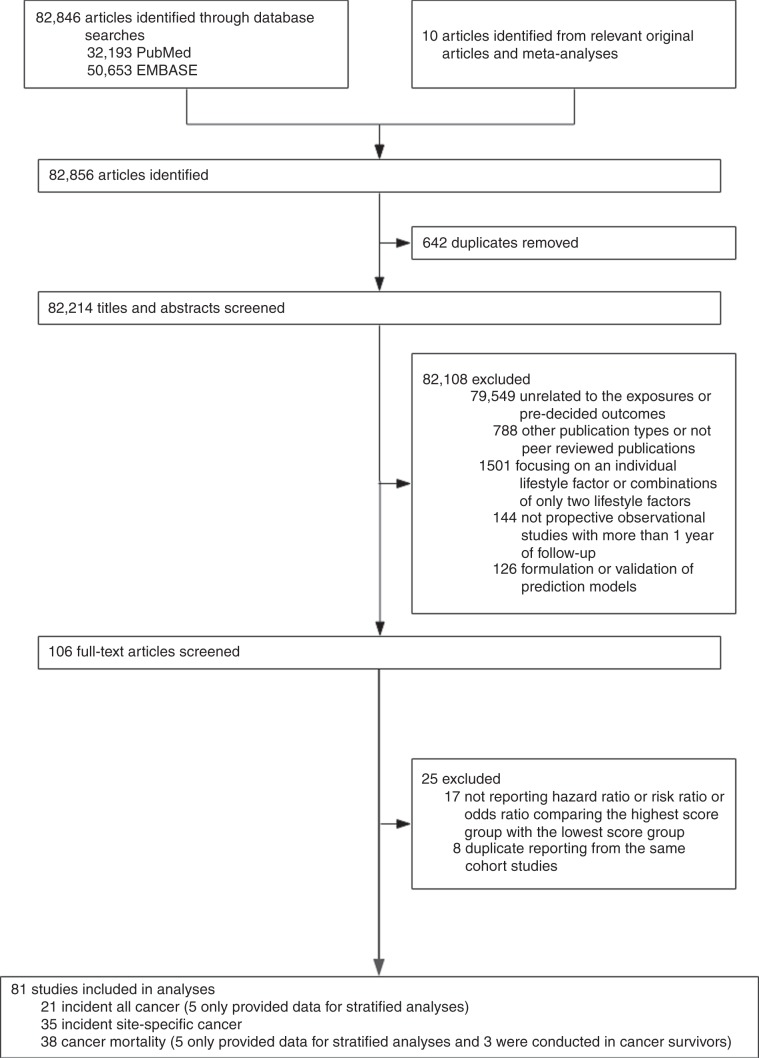
Methods: EMBASE and PubMed were searched up to April 2019. Cohort studies investigating the association of combined lifestyle factors with risks of incident cancer and cancer mortality were selected. Summary hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated using random-effects models. Heterogeneity and publication bias tests were conducted.
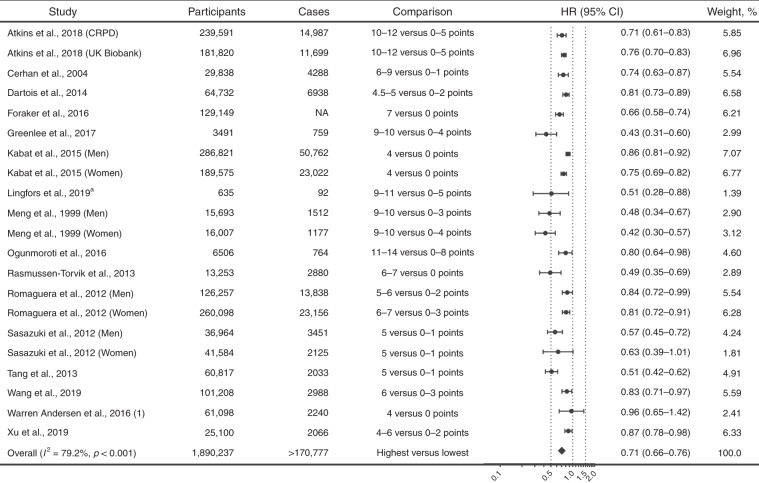
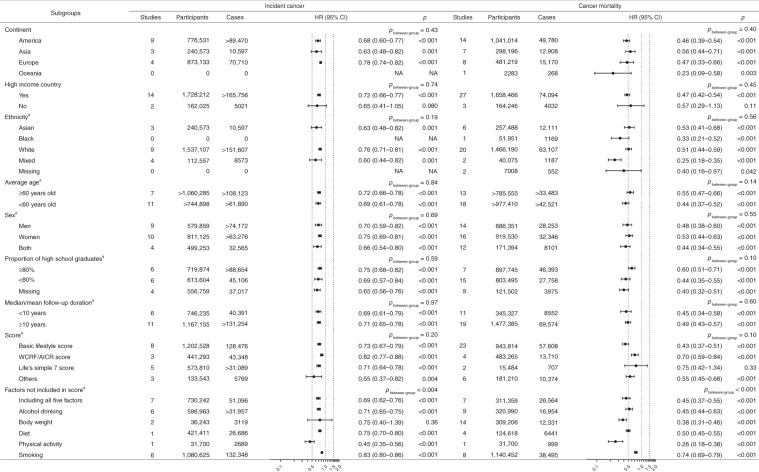
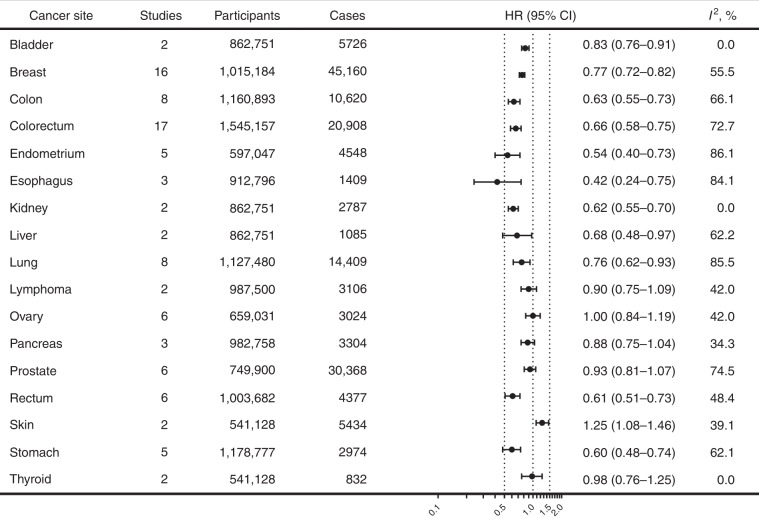
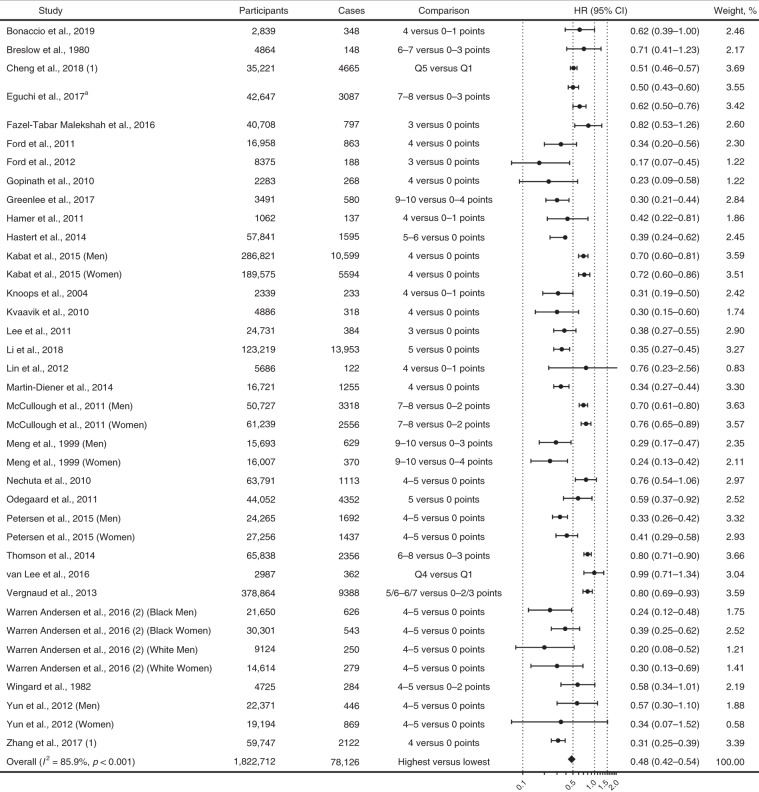
Results: The HRs (95% CIs) comparing individuals with the healthiest versus the least healthy lifestyles were 0.71 (0.66-0.76; 16 studies with 1.9 million participants) for incident cancer and 0.48 (0.42-0.54; 30 studies with 1.8 million participants) for cancer mortality. Adopting the healthiest lifestyles was also associated with 17 to 58% lower risks of bladder, breast, colon, endometrial, oesophageal, kidney, liver, lung, rectal, and gastric cancer. The relations were largely consistent and significant among participants with different characteristics in the subgroup analyses.
Conclusions: Adopting healthy lifestyles is associated with substantial risk reduction in cancer morbidity and mortality, and thus should be given priority for cancer prevention.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Kyu HH, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1859–1922. doi: 10.1016/S0140-6736(18)32335-3. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
