

Epidemiology of Pediatric Traumatic Brain Injury and Hypothalamic-Pituitary Disorders in Arizona
- PMID: 32038466
- PMCID: PMC6988738
- DOI: 10.3389/fneur.2019.01410
Epidemiology of Pediatric Traumatic Brain Injury and Hypothalamic-Pituitary Disorders in Arizona
Abstract
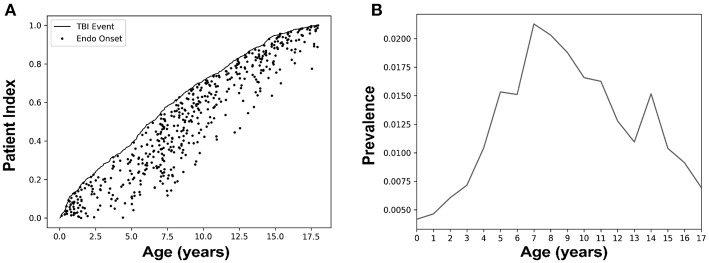
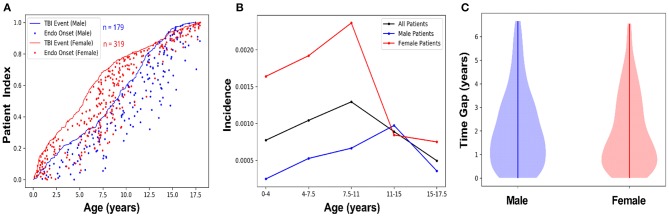
Traumatic brain injury (TBI) in children can result in long-lasting social, cognitive, and neurological impairments. In adults, TBI can lead to endocrinopathies (endocrine system disorders), but this is infrequently reported in children. Untreated endocrinopathies can elevate risks of subsequent health issues, such that early detection in pediatric TBI survivors can initiate clinical interventions. To understand the risk of endocrinopathies following pediatric TBI, we identified patients who had experienced a TBI and subsequently developed a new-onset hypothalamic regulated endocrinopathy (n = 498). We hypothesized that pediatric patients who were diagnosed with a TBI were at higher risk of being diagnosed with a central endocrinopathy than those without a prior diagnosis of TBI. In our epidemiological assessment, we identified pediatric patients enrolled in the Arizona Health Care Cost Containment System (AHCCCS) from 2008 to 2014 who were diagnosed with one of 330 TBI International Classification of Diseases (ICD)-9 codes and subsequently diagnosed with one of 14 central endocrinopathy ICD-9 codes. Additionally, the ICD-9 code data from over 600,000 Arizona pediatric patients afforded an estimate of the incidence, prevalence, relative risk, odds ratio, and number needed to harm, regarding the development of a central endocrinopathy after sustaining a TBI in Arizona Medicaid pediatric patients. Children with a TBI diagnosis had 3.22 times the risk of a subsequent central endocrine diagnosis compared with the general population (±0.28). Pediatric AHCCCS patients with a central endocrine diagnosis had 3.2-fold higher odds of a history of a TBI diagnosis than those without an endocrine diagnosis (±0.29). Furthermore, the number of patients with a TBI diagnosis for one patient to receive a diagnosis of a central endocrine diagnosis was 151.2 (±6.12). Female subjects were more likely to present with a central endocrine diagnosis after a TBI diagnosis compared to male subjects (64.1 vs. 35.9%). These results are the first state-wide epidemiological study conducted to determine the risk of developing a hypothalamic-pituitary disorder after a TBI in the pediatric population. Our results contribute to a body of knowledge demonstrating a TBI etiology for idiopathic endocrine disorders, and thus advise physicians with regard to TBI follow-up care that includes preventive screening for endocrine disorders.
Keywords: adolescence; concussion; endocrine dysfunction; head injury; hypopituitarism; pediatrics; puberty; traumatic brain injury.
Copyright © 2020 Ortiz, Sukhina, Balkan, Harootunian, Adelson, Lewis, Oatman, Subbian, Rowe and Lifshitz.
Figures
References
-
- Faul M, Wald MM, Xu L, Coronado VG. Traumatic Brain Injury in the United States; Emergency Department Visits, Hospitalizations, and Deaths 2002–2006. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control; (2010).
LinkOut - more resources
Full Text Sources