

New treatments/targets for primary biliary cholangitis
- PMID: 32039371
- PMCID: PMC7001536
- DOI: 10.1016/j.jhepr.2019.05.005
New treatments/targets for primary biliary cholangitis
Abstract
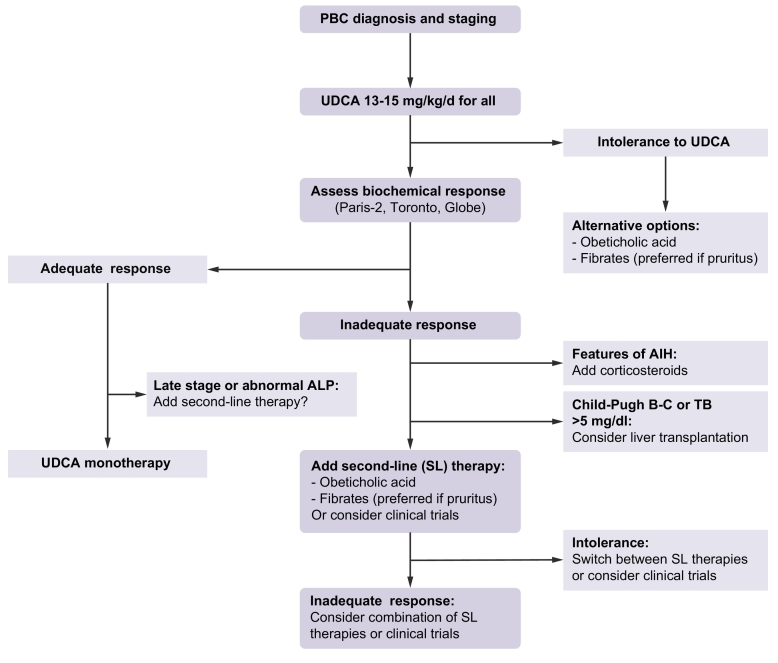
Primary biliary cholangitis (PBC) is an autoimmune, cholestatic, chronic liver disease that ultimately progresses towards cirrhosis and liver failure if untreated. While ursodeoxycholic acid has been established as standard of care for PBC in the last few decades, significant advances in second-line treatment options have recently been made and new therapeutic developments are currently under evaluation. The purpose of this article is to provide the clinician with an overview of the current treatment options and future opportunities for patients with PBC.
Keywords: FXR; PBC; PPAR; cholestasis; fibrates; inflammation; liver disease; obeticholic acid; ursodeoxycholic acid.
© 2019 The Author(s).
Figures
References
-
- EASL Clinical Practice Guidelines: The diagnosis and management of patients with primary biliary cholangitisJ Hepatol. 2017;67:145–172. - PubMed
-
- Lindor KD, Bowlus CL, Boyer J, Levy C, Mayo M. Primary Biliary Cholangitis: 2018 Practice Guidance from the American Association for the Study of Liver Diseases. Hepatology. 2019;69:394–419. - PubMed
-
- Harms MH, van Buuren HR, Corpechot C, Thorburn D, Janssen HLA, Lindor KD. Ursodeoxycholic acid therapy and liver transplant-free survival in patients with primary biliary cholangitis. J Hepatol. 2019;71:357–365. Epub 2019 Apr 11. - PubMed
-
- Pares A, Caballeria L, Rodes J. Excellent long-term survival in patients with primary biliary cirrhosis and biochemical response to ursodeoxycholic Acid. Gastroenterology. 2006;130:715–720. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
