

Anchorless Arthroscopic Transosseous and Anchored Arthroscopic Transosseous Equivalent Rotator Cuff Repair Show No Differences in Structural Integrity or Patient-reported Outcomes in a Matched Cohort
- PMID: 32039957
- PMCID: PMC7319398
- DOI: 10.1097/CORR.0000000000001151
Anchorless Arthroscopic Transosseous and Anchored Arthroscopic Transosseous Equivalent Rotator Cuff Repair Show No Differences in Structural Integrity or Patient-reported Outcomes in a Matched Cohort
Abstract
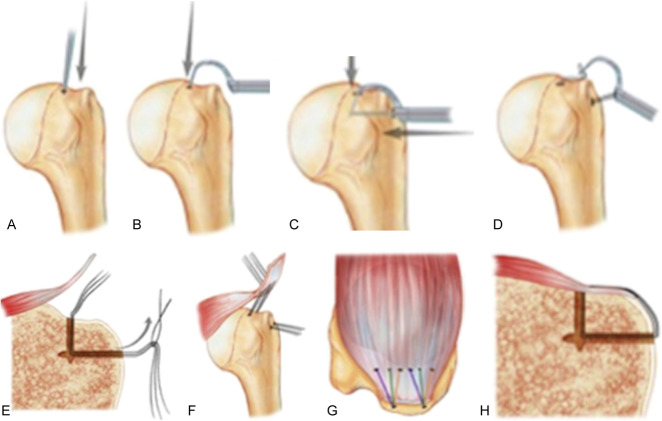
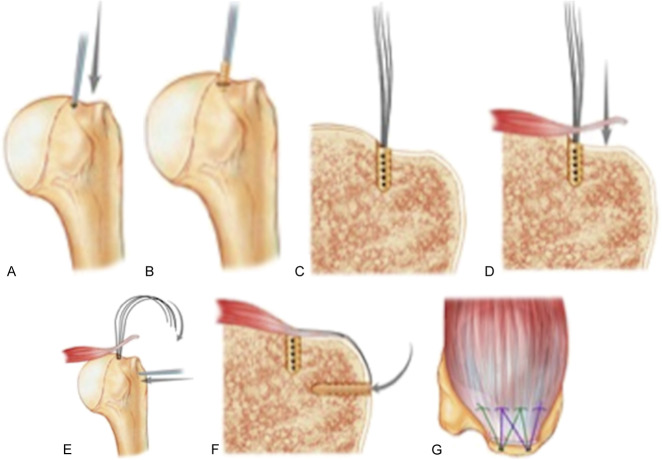
Background: Anchored transosseous equivalent suture-bridge technique (TOE) is widely used for arthroscopic rotator cuff repair. It is unknown how patient outcomes scores, ROM, and integrity of the rotator cuff after repair using this anchored technique compare with those after repair using an anchorless transosseous technique (TO).
Questions/purposes: (1) What are the differences in patient-reported outcomes (American Shoulder and Elbow Surgeons [ASES] score) and shoulder ROM between TO and TOE rotator cuff repair techniques at 1 and 2 years after surgery? (2) What is the difference in repair integrity as measured by the re-tear rate, assessed ultrasonographically at 1 year, between these two techniques? (3) What is the difference in procedure duration between the two techniques when performed by a surgeon familiar with each?
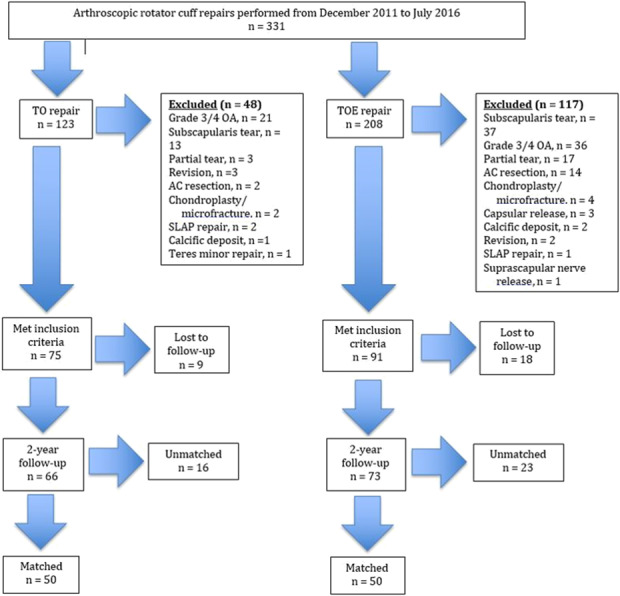
Methods: We reviewed 331 arthroscopic rotator cuff repairs performed by one surgeon from December 2011 to July 2016 in this retrospective, matched-pair study. Of these patients, 63% (208 of 331) underwent repair with standard anchored technique (anchors placed in a double-row, TOE manner) and 37% (123 of 331) underwent anchorless TO repair, with the same indications for surgery between groups. Forty-four percent (91 of 208) of patients in the TOE group and 61% (75 of 123) of patients in the TO group met the inclusion criteria. Eighty percent (73 of 91) of patients in the TOE group and 88% (66 of 75) in the TO group had minimum 2-year follow-up. We matched each group to a cohort of 50 patients by sex, age, smoking status, and tear size (by Cofield classification: small, < 1 cm; medium, 1-3 cm; large, > 3-5 cm; or massive, > 5 cm). The resulting cohorts did not differ in mean age (TO, 62 years [range 53-65 years]; TOE, 58 years [range 53-65 years]; p = 0.79), mean BMI value (TO, 30 [range 27-33]; TOE, 29 [range 27-35]; p = 0.97), or dominant arm involvement (TO, 80%; TOE, 78%; p = 0.81). The cohorts were followed for at least 2 years (median, 3.2 years [interquartile range (IQR) 2.2-4.3] for TO and 2.9 years [IQR 2.0-3.5 years] for TOE). ASES scores and ROM were evaluated before surgery and at follow-up visits and were recorded in a longitudinally maintained institutional database. Repair integrity was assessed using ultrasonography at 1 year, as is standard in our practice. For each tear-size group, we calculated the proportion of intact tendon repairs versus the proportion of re-tears. Duration of surgery was recorded for each patient.
Results: At 1 year, we observed no difference in median ASES scores (90 [IQR 92-98] for TO and 88 [IQR 72-98] for TOE; p = 0.44); external rotation (50° [IQR 45°-60°) for TO and 50° [IQR: 40°-60°] for TOE; p = 0.58); forward flexion (165° [IQR 160°-170°] for both groups; p = 0.91); or abduction (100° [IQR 90°-100°] for TO and 90° [IQR 90°-100°] for TOE; p = 0.06). Fourteen percent of shoulders (seven of 50) in each treatment group had evidence of re-tear at 1 year (p > 0.99): 0 of 2 small tears in each group, 0 of 7 medium tears in each group, five of 32 large tears in each group, and two of 9 massive tears in each group (all, p > 0.99). At 2 years, we found no differences in median ASES scores (92 [IQR 74-98)] for TO and 90 [IQR 80-100] for TOE; p = 0.84); external rotation (60° [IQR 50°-60°] for both groups; p = 0.74); forward flexion (170° [IQR 160°-170°] for both groups; p = 0.69); or abduction (100° [IQR 90°-100°] for both groups; p = 0.95). We found no differences between groups in mean ± SD procedure time, which was 103 ± 20 minutes for TO repair and 99 ± 20 minutes for TOE repair (p = 0.45).
Conclusions: TO and TOE techniques for arthroscopic rotator cuff repair results in no differences in ROM, ASES scores, re-tear rates, and surgical time. Randomized control trials are needed to confirm these similarities or determine a superior method of repair. Future cost analyses may also help to determine the relative value of each technique.
Level of evidence: Level III, therapeutic study.
Conflict of interest statement
Each of the remaining authors certifies that neither he or she, nor any member of his or her immediate family, have funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: Anchorless Arthroscopic Transosseous and Anchored Arthroscopic Transosseous Equivalent Rotator Cuff Repair Show No Differences in Structural Integrity or Patient-reported Outcomes in a Matched Cohort.Clin Orthop Relat Res. 2020 Jun;478(6):1304-1306. doi: 10.1097/CORR.0000000000001253. Clin Orthop Relat Res. 2020. PMID: 32282536 Free PMC article. No abstract available.
References
-
- Apreleva M, Ozbaydar M, Fitzgibbons PG, Warner JJ. Rotator cuff tears: the effect of the reconstruction method on three-dimensional repair site area. Arthroscopy. 2002;18:519-526. - PubMed
-
- Behrens SB, Bruce B, Zonno AJ, Paller D, Green A. Initial fixation strength of transosseous-equivalent suture bridge rotator cuff repair is comparable with transosseous repair. Am. J. Sports Med. 2012;40:133-140. - PubMed
-
- Brigham and Women's Hospital. Arthroscopic Rotator Cuff Repair Frequently Asked Questions. Available at: https://www.brighamandwomens.org/assets/BWH/patients-and-families/rehabi.... Accessed on November 26. 2016.
-
- Cho NS, Yi JW, Lee BG, Rhee YG. Retear patterns after arthroscopic rotator cuff repair: single-row versus suture bridge technique. Am J Sports Med. 2010;38:664-671. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
