

Disparities of National Lung Cancer Screening Guidelines in the US Population
- PMID: 32040195
- PMCID: PMC7669226
- DOI: 10.1093/jnci/djaa013
Disparities of National Lung Cancer Screening Guidelines in the US Population
Abstract
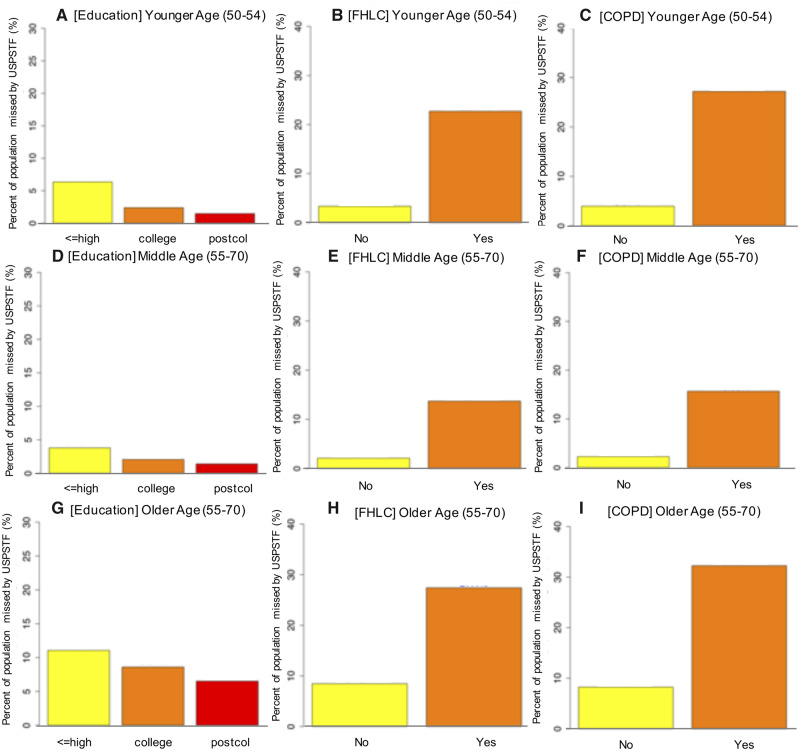
Background: Current US Preventive Services Task Force (USPSTF) lung cancer screening guidelines are based on smoking history and age (55-80 years). These guidelines may miss those at higher risk, even at lower exposures of smoking or younger ages, because of other risk factors such as race, family history, or comorbidity. In this study, we characterized the demographic and clinical profiles of those selected by risk-based screening criteria but were missed by USPSTF guidelines in younger (50-54 years) and older (71-80 years) age groups.
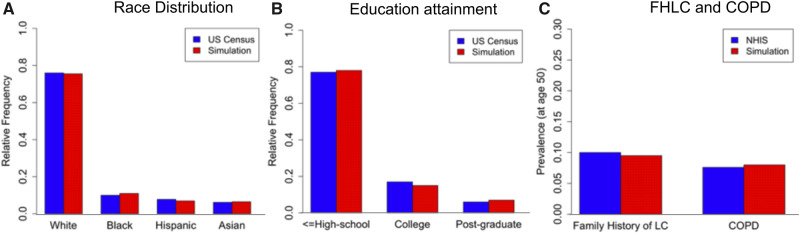
Methods: We used data from the National Health Interview Survey, the CISNET Smoking History Generator, and results of logistic prediction models to simulate lifetime lung cancer risk-factor data for 100 000 individuals in the 1950-1960 birth cohorts. We calculated age-specific 6-year lung cancer risk for each individual from ages 50 to 90 years using the PLCOm2012 model and evaluated age-specific screening eligibility by USPSTF guidelines and by risk-based criteria (varying thresholds between 1.3% and 2.5%).
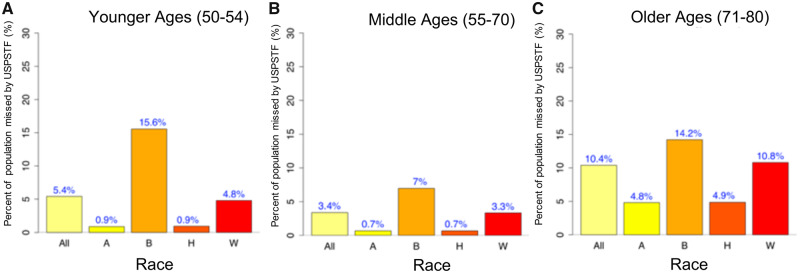
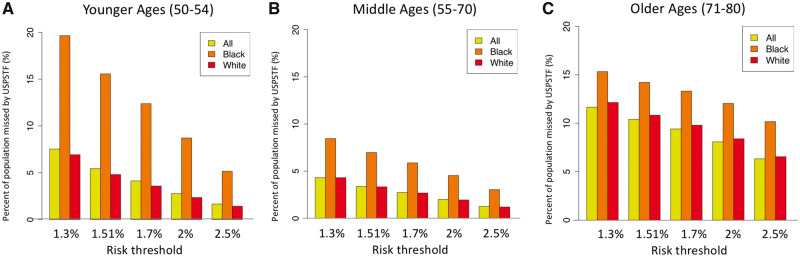
Results: In the 1950 birth cohort, 5.4% would have been ineligible for screening by USPSTF criteria in their younger ages but eligible based on risk-based criteria. Similarly, 10.4% of the cohort would be ineligible for screening by USPSTF in older ages. Notably, high proportions of blacks were ineligible for screening by USPSTF criteria at younger (15.6%) and older (14.2%) ages, which were statistically significantly greater than those of whites (4.8% and 10.8%, respectively; P < .001). Similar results were observed with other risk thresholds and for the 1960 cohort.
Conclusions: Further consideration is needed to incorporate comprehensive risk factors, including race and ethnicity, into lung cancer screening to reduce potential racial disparities.
© The Author(s) 2020. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Similar articles
-
Addressing Sex Disparities in Lung Cancer Screening Eligibility: USPSTF vs PLCOm2012 Criteria.Chest. 2022 Jan;161(1):248-256. doi: 10.1016/j.chest.2021.06.066. Epub 2021 Jul 9. Chest. 2022. PMID: 34252436
-
The 2021 US Preventive Services Task Force lung cancer screening eligibility criteria disproportionately exclude younger Black patients with lung cancer.Cancer. 2025 Jan 1;131(1):e35676. doi: 10.1002/cncr.35676. Epub 2024 Dec 11. Cancer. 2025. PMID: 39660785
-
Risk Model-Based Lung Cancer Screening and Racial and Ethnic Disparities in the US.JAMA Oncol. 2023 Dec 1;9(12):1640-1648. doi: 10.1001/jamaoncol.2023.4447. JAMA Oncol. 2023. PMID: 37883107 Free PMC article.
-
Evaluation of the Benefits and Harms of Lung Cancer Screening With Low-Dose Computed Tomography: A Collaborative Modeling Study for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2021 Mar. Report No.: 20-05266-EF-2. Rockville (MD): Agency for Healthcare Research and Quality (US); 2021 Mar. Report No.: 20-05266-EF-2. PMID: 33750088 Free Books & Documents. Review.
-
The Patient Perspective on Lung Cancer Screening and Health Disparities.J Am Coll Radiol. 2019 Apr;16(4 Pt B):601-606. doi: 10.1016/j.jacr.2018.12.028. J Am Coll Radiol. 2019. PMID: 30947894 Review.
Cited by
-
Lung Cancer Screening in Brazil Comparing the 2013 and 2021 USPSTF Guidelines.JAMA Netw Open. 2023 Dec 1;6(12):e2346994. doi: 10.1001/jamanetworkopen.2023.46994. JAMA Netw Open. 2023. PMID: 38079172 Free PMC article.
-
Impact of U.S. Preventive Services Task Force lung cancer screening update on drivers of disparities in screening eligibility.Cancer Med. 2023 Feb;12(4):4647-4654. doi: 10.1002/cam4.5066. Epub 2022 Jul 24. Cancer Med. 2023. PMID: 35871312 Free PMC article.
-
Racial and Ethnic Bias in Risk Prediction Models for Colorectal Cancer Recurrence When Race and Ethnicity Are Omitted as Predictors.JAMA Netw Open. 2023 Jun 1;6(6):e2318495. doi: 10.1001/jamanetworkopen.2023.18495. JAMA Netw Open. 2023. PMID: 37318804 Free PMC article.
-
Disparities in thoracic surgical oncology.J Surg Oncol. 2023 Feb;127(2):329-335. doi: 10.1002/jso.27180. J Surg Oncol. 2023. PMID: 36630104 Free PMC article. Review.
-
Lung cancer screening use and implications of varying eligibility criteria by race and ethnicity: 2019 Behavioral Risk Factor Surveillance System data.Cancer. 2022 May 1;128(9):1812-1819. doi: 10.1002/cncr.34098. Epub 2022 Feb 24. Cancer. 2022. PMID: 35201610 Free PMC article.
References
-
- Moyer VA. Screening for lung cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(5):330–338. - PubMed
-
- Li C-C, Matthews AK, Rywant MM, et al. Racial disparities in eligibility for low-dose computed tomography lung cancer screening among older adults with a history of smoking. Cancer Causes Control. 2019;30(3):235–240. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
