

Quantitative 18F-FDG PET-CT scan characteristics correlate with tuberculosis treatment response
- PMID: 32040770
- PMCID: PMC7010890
- DOI: 10.1186/s13550-020-0591-9
Quantitative 18F-FDG PET-CT scan characteristics correlate with tuberculosis treatment response
Abstract
Background: There is a growing interest in the use of F-18 FDG PET-CT to monitor tuberculosis (TB) treatment response. Tuberculosis lung lesions are often complex and diffuse, with dynamic changes during treatment and persisting metabolic activity after apparent clinical cure. This poses a challenge in quantifying scan-based markers of burden of disease and disease activity. We used semi-automated, whole lung quantification of lung lesions to analyse serial FDG PET-CT scans from the Catalysis TB Treatment Response Cohort to identify characteristics that best correlated with clinical and microbiological outcomes.
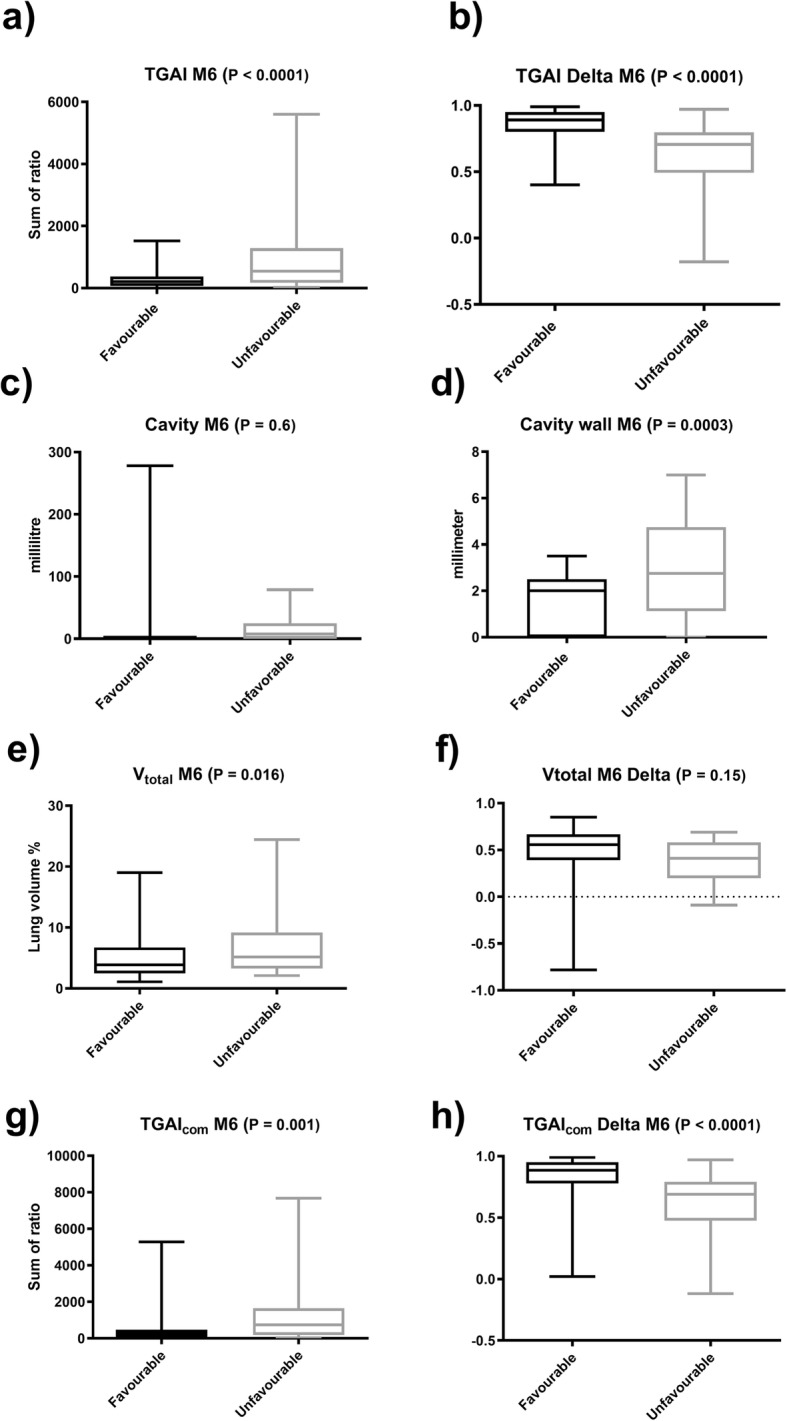
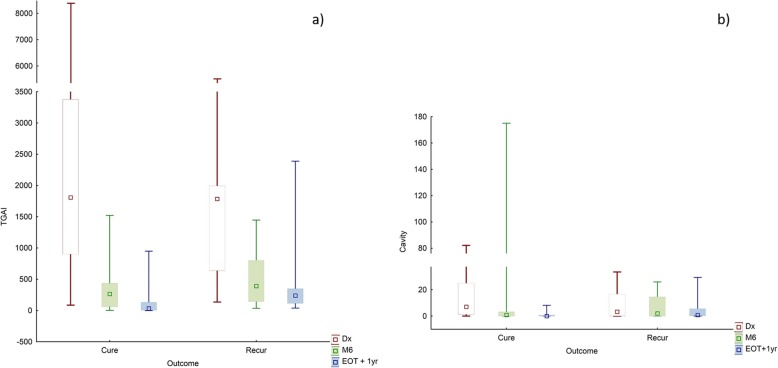
Results: Quantified scan metrics were already associated with clinical outcomes at diagnosis and 1 month after treatment, with further improved accuracy to differentiate clinical outcomes after standard treatment duration (month 6). A high cavity volume showed the strongest association with a risk of treatment failure (AUC 0.81 to predict failure at diagnosis), while a suboptimal reduction of the total glycolytic activity in lung lesions during treatment had the strongest association with recurrent disease (AUC 0.8 to predict pooled unfavourable outcomes). During the first year after TB treatment lesion burden reduced; but for many patients, there were continued dynamic changes of individual lesions.
Conclusions: Quantification of FDG PET-CT images better characterised TB treatment outcomes than qualitative scan patterns and robustly measured the burden of disease. In future, validated metrics may be used to stratify patients and help evaluate the effectiveness of TB treatment modalities.
Keywords: 18F-FDG; Mycobacterium tuberculosis; PET-CT; Quantified lung analysis; Quantitative imaging analysis; Tuberculosis; Tuberculosis treatment response.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- WHO . Global tuberculosis report 2018. 2018.
-
- Wejse C, Gustafson P, Nielsen J, Gomes VF, Aaby P, Andersen PL, Sodemann M. TBscore: signs and symptoms from tuberculosis patients in a low-resource setting have predictive value and may be used to assess clinical course. Scand J Infect Dis. 2008;40(2):111–120. doi: 10.1080/00365540701558698. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
