

Neurally adjusted ventilatory assist vs. pressure support to deliver protective mechanical ventilation in patients with acute respiratory distress syndrome: a randomized crossover trial
- PMID: 32040785
- PMCID: PMC7010869
- DOI: 10.1186/s13613-020-0638-0
Neurally adjusted ventilatory assist vs. pressure support to deliver protective mechanical ventilation in patients with acute respiratory distress syndrome: a randomized crossover trial
Abstract
Background: Protective mechanical ventilation is recommended for patients with acute respiratory distress syndrome (ARDS), but it usually requires controlled ventilation and sedation. Using neurally adjusted ventilatory assist (NAVA) or pressure support ventilation (PSV) could have additional benefits, including the use of lower sedative doses, improved patient-ventilator interaction and shortened duration of mechanical ventilation. We designed a pilot study to assess the feasibility of keeping tidal volume (VT) at protective levels with NAVA and PSV in patients with ARDS.
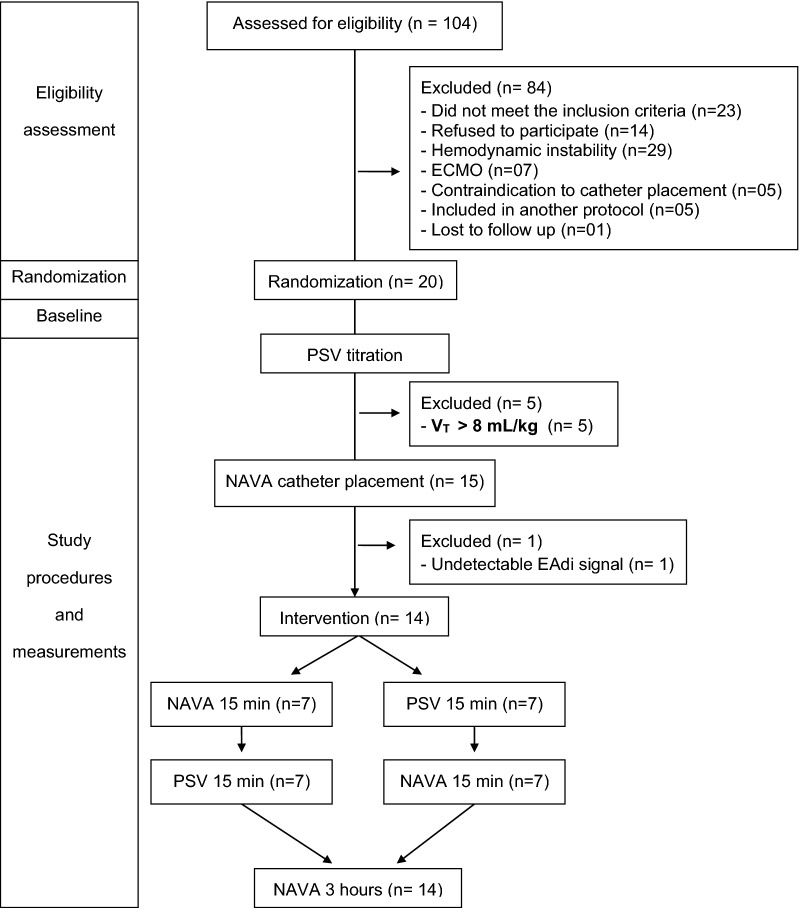
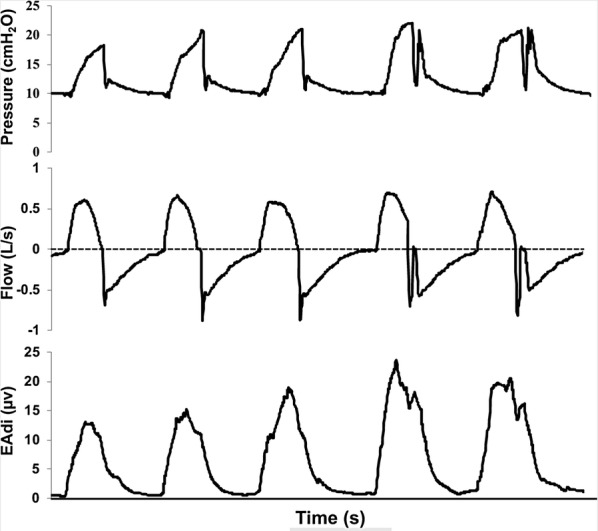
Methods: We conducted a prospective randomized crossover trial in five ICUs from a university hospital in Brazil and included patients with ARDS transitioning from controlled ventilation to partial ventilatory support. NAVA and PSV were applied in random order, for 15 min each, followed by 3 h in NAVA. Flow, peak airway pressure (Paw) and electrical activity of the diaphragm (EAdi) were captured from the ventilator, and a software (Matlab, Mathworks, USA), automatically detected inspiratory efforts and calculated respiratory rate (RR) and VT. Asynchrony events detection was based on waveform analysis.
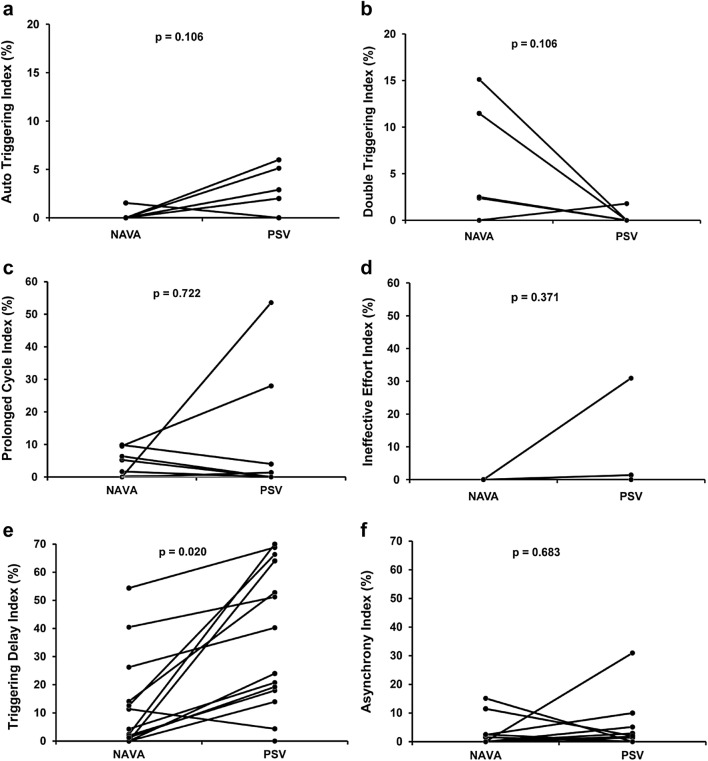
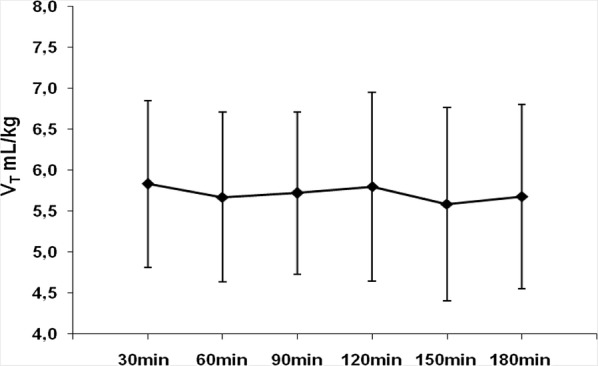
Results: We randomized 20 patients, but the protocol was interrupted for five (25%) patients for whom we were unable to maintain VT below 6.5 mL/kg in PSV due to strong inspiratory efforts and for one patient for whom we could not detect EAdi signal. For the 14 patients who completed the protocol, VT was 5.8 ± 1.1 mL/kg for NAVA and 5.6 ± 1.0 mL/kg for PSV (p = 0.455) and there were no differences in RR (24 ± 7 for NAVA and 23 ± 7 for PSV, p = 0.661). Paw was greater in NAVA (21 ± 3 cmH2O) than in PSV (19 ± 3 cmH2O, p = 0.001). Most patients were under continuous sedation during the study. NAVA reduced triggering delay compared to PSV (p = 0.020) and the median asynchrony Index was 0.7% (0-2.7) in PSV and 0% (0-2.2) in NAVA (p = 0.6835).
Conclusions: It was feasible to keep VT in protective levels with NAVA and PSV for 75% of the patients. NAVA resulted in similar VT, RR and Paw compared to PSV. Our findings suggest that partial ventilatory assistance with NAVA and PSV is feasible as a protective ventilation strategy in selected ARDS patients under continuous sedation. Trial registration ClinicalTrials.gov (NCT01519258). Registered 26 January 2012, https://clinicaltrials.gov/ct2/show/NCT01519258.
Keywords: Interactive ventilatory support; Neurally adjusted ventilatory assist; Positive-pressure respiration; Respiration, artificial; Respiratory distress syndrome, adult.
Conflict of interest statement
Dr. Juliana Ferreira received fees for lecturing from Medtronic from 2016 to 2019. Dr. Marcelo B.P. Amato, MD, reports that his research laboratory has received grants in the last 5 years from the Covidien/Medtronic (mechanical ventilation), Orange Med/Nihon Kohden (mechanical ventilation) and Timpel S.A (Electrical Impedance Tomography). Dr. Marcelo B.P. Amato is also a minority shareholder in Timpel. The authors, FDS, HTM, AML, and CRRC have no conflicts of interest to disclose related to the contents of the manuscript.
Figures
References
-
- Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;195:1253–1263. doi: 10.1164/rccm.201703-0548ST. - DOI - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
