

Adherence to the SEP-1 Sepsis Bundle in Hospital-Onset v. Community-Onset Sepsis: a Multicenter Retrospective Cohort Study
- PMID: 32040837
- PMCID: PMC7174506
- DOI: 10.1007/s11606-020-05653-0
Adherence to the SEP-1 Sepsis Bundle in Hospital-Onset v. Community-Onset Sepsis: a Multicenter Retrospective Cohort Study
Abstract
Background: Sepsis is the leading cause of in-hospital death. The SEP-1 sepsis bundle is a protocol for early sepsis care that requires providers to diagnose and treat sepsis quickly. Limited evidence suggests that adherence to the sepsis bundle is lower in cases of hospital-onset sepsis.
Objective: To compare sepsis bundle adherence in hospital-onset vs. community-onset sepsis.
Design: Retrospective cohort study using multivariable analysis of clinical data.
Participants: A total of 4658 inpatients age 18 or older were identified by diagnosis codes consistent with sepsis or disseminated infection.
Setting: Four university hospitals in California between 2014 and 2016.
Main outcomes and measures: The primary outcome was adherence to key components of the sepsis bundle defined by the Centers for Medicare and Medicaid Services in their core measure, SEP-1. Covariates included clinical characteristics related to the patient, infection, and pathogen.
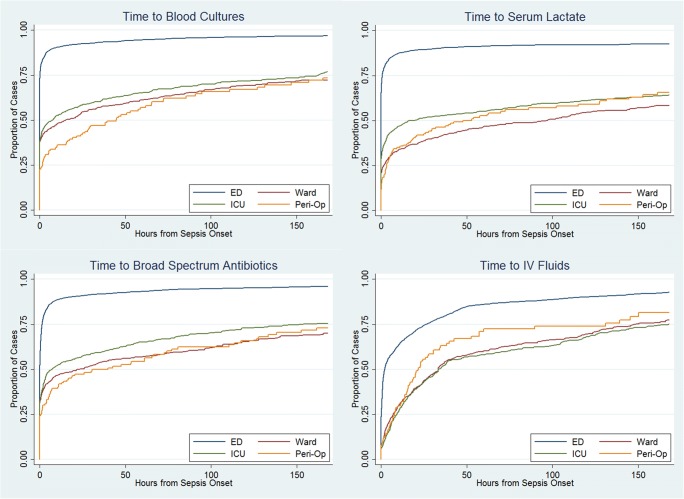
Key results: Compared with community-onset, cases of hospital-onset sepsis were less likely to receive SEP-1 adherent care (relative risk 0.33, 95% confidence interval 0.29-0.38, p < 0.001). With the exception of vasopressors (RR 1.11, p = 0.002), each component of SEP-1 evaluated-blood cultures (RR 0.76, p < 0.001), serum lactate (RR 0.51, p < 0001), broad-spectrum antibiotics (RR 0.62, p < 0.001), intravenous fluids (0.47, p < 0.001), and follow-up lactate (RR 0.71, p < 0.001)-was less likely to be performed within the recommended time frame in hospital-onset sepsis. Within the hospital, cases of hospital-onset sepsis arising on the ward were less likely to receive SEP-1-adherent care than were cases arising in the intensive care unit (RR 0.68, p = 0.004).
Conclusions: Inpatients with hospital-onset sepsis receive different management than individuals with community-onset sepsis. It remains to be determined whether system-level factors, provider-level factors, or factors related to measurement explain the observed variation in care or whether variation in care affects outcomes.
Keywords: critical care; health services research; hospital medicine; infectious disease; performance measurement.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures

References
-
- Elixhauser, A., Friedman, B, Stranges, E. Septicemia in U.S. Hospitals, 2009. Healthcare Cost and Utilization Project, Statical Brief #122. 2011 [December 6, 2019]; Available from: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb122.pdf.
-
- Novosad, S.A., Vital signs: epidemiology of sepsis: prevalence of health care factors and opportunities for prevention. MMWR. Morbidity and mortality weekly report, 2016. 65. - PubMed
