

Socioeconomic Inequities in Adherence to Positive Airway Pressure Therapy in Population-Level Analysis
- PMID: 32041146
- PMCID: PMC7074027
- DOI: 10.3390/jcm9020442
Socioeconomic Inequities in Adherence to Positive Airway Pressure Therapy in Population-Level Analysis
Abstract
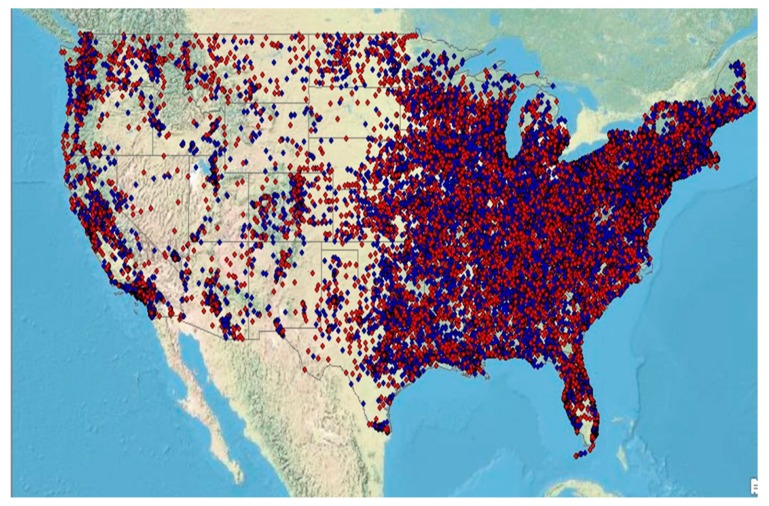
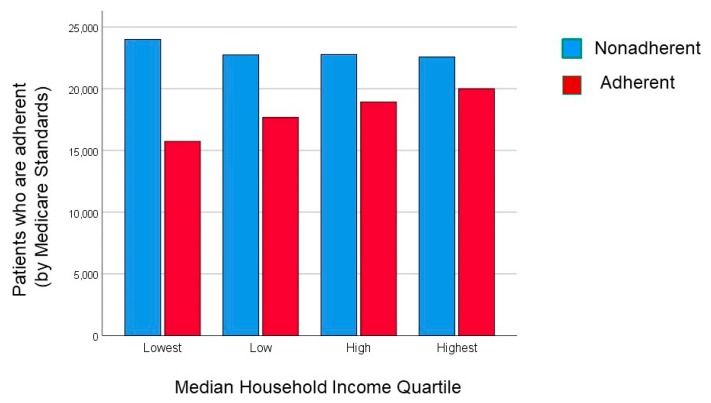
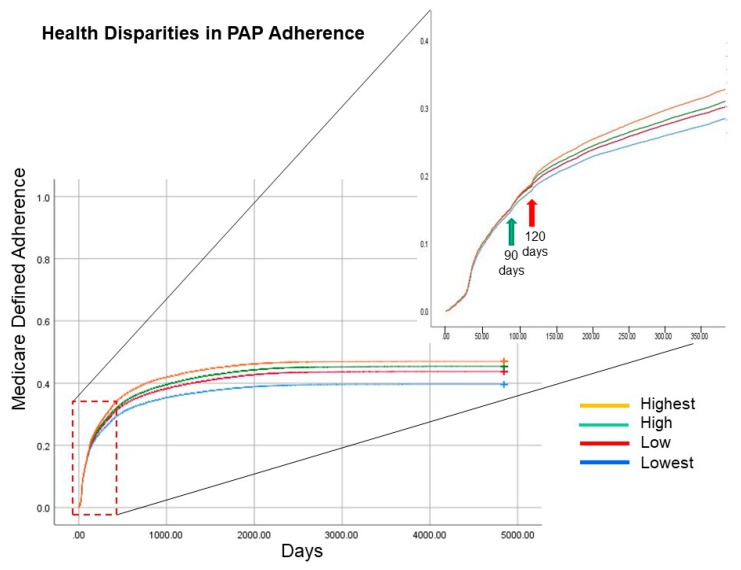
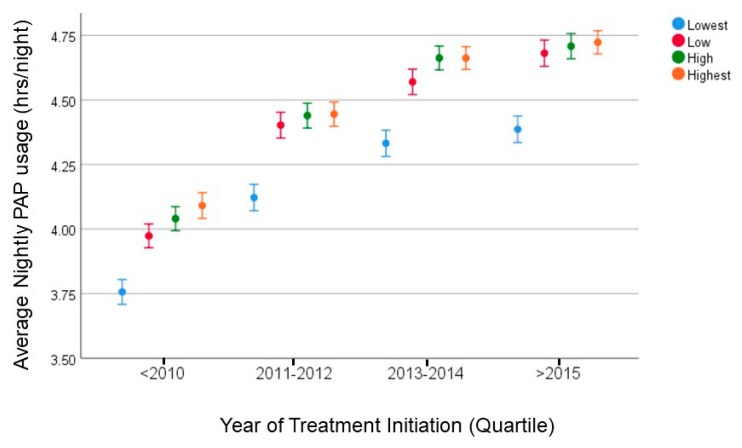
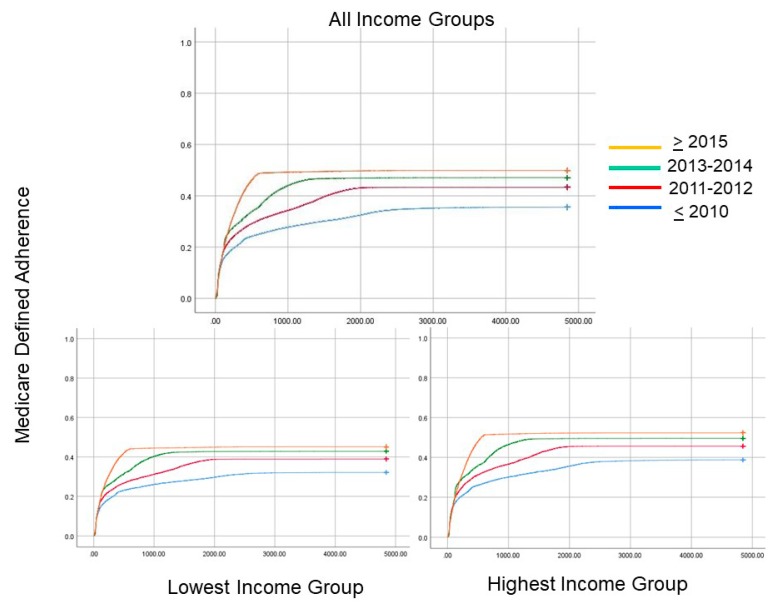
(a) Background: In patients with sleep apnea, poor adherence to positive airway pressure (PAP) therapy has been associated with mortality. Regional studies have suggested that lower socioeconomic status is associated with worse PAP adherence but population-level data is lacking. (b) Methods: De-identified data from a nationally representative database of PAP devices was geo-linked to sociodemographic information. (c) Results: In 170,641 patients, those in the lowest quartile of median household income had lower PAP adherence (4.1 + 2.6 hrs/night; 39.6% adherent by Medicare criteria) than those in neighborhoods with highest quartile median household income (4.5 + 2.5 hrs/night; 47% adherent by Medicare criteria; p < 0.0001). In multivariate regression, individuals in neighborhoods with the highest income quartile were more adherent to PAP therapy than those in the lowest income quartile after adjusting for various confounders (adjusted Odds Ratio (adjOR) 1.18; 95% confidence interval (CI) 1.14, 1.21; p < 0.0001). Over the past decade, PAP adherence improved over time (adjOR 1.96; 95%CI 1.94, 2.01), but health inequities in PAP adherence remained even after the Affordable Care Act was passed. (d) Conclusion: In a nationally representative population, disparities in PAP adherence persist despite Medicaid expansion. Interventions aimed at promoting health equity in sleep apnea need to be undertaken.
Keywords: adherence; big data; health disparities; health equity; health policy; positive airway pressure therapy; sleep apnea.
Conflict of interest statement
The funding institution did not have any role in the design, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. Parthasarathy reports grants from NIH/NHLBI (HL095799 and HL095748), grants from Patient Centered Outcomes Research Institute (IHS-1306-2505, EAIN #3394-UoA, and PPRND-1507-31666), grants from US Department of Defense, grants from NIH (National Cancer Institute; R21CA184920), grants from Johrei Institute, personal fees from American Academy of Sleep Medicine, personal fees from American College of Chest Physicians, non-financial support from National Center for Sleep Disorders Research of the NIH (NHLBI), personal fees from UpToDate Inc., Philips-Respironics, Inc., and Vaopotherm, Inc.; grants from Younes Sleep Technologies, Ltd., Niveus Medical Inc., and Philips-Respironics, Inc. outside the submitted work. In addition, Parthasarathy has a patent UA 14-018 U.S.S.N. 61/884,654; PTAS 502570970 (home breathing device). The above-mentioned conflicts including the patent are unrelated to the topic of this paper. Combs has research grants from the American Sleep Medicine Foundation and NIH/NHLBI (R61HL151254). Patel has a research grant from the American Sleep Medicine Foundation. Seixas is funded by the NIH/NHLBI (K01HL135452) and Merck Inc. Jean-Louis is funded by NIH/NHLBI (R01HL142066, R25NS094093) and NIH/NIA (R01AG056531). The authors have no conflict of interest to disclose.
Figures
Similar articles
-
The Effect of Sleeping Environment and Sleeping Location Change on Positive Airway Pressure Adherence.J Clin Sleep Med. 2018 Oct 15;14(10):1645-1652. doi: 10.5664/jcsm.7364. J Clin Sleep Med. 2018. PMID: 30353802 Free PMC article.
-
Centers for Medicare and Medicaid Services Positive Airway Pressure Adherence Criteria May Limit Treatment to Many Medicare Beneficiaries.J Clin Sleep Med. 2019 Feb 15;15(2):245-251. doi: 10.5664/jcsm.7626. J Clin Sleep Med. 2019. PMID: 30736874 Free PMC article.
-
Adherence and Subthreshold Adherence in Sleep Apnea Subjects Receiving Positive Airway Pressure Therapy: A Retrospective Study Evaluating Differences in Adherence Versus Use.Respir Care. 2016 Aug;61(8):1023-32. doi: 10.4187/respcare.04538. Epub 2016 Apr 26. Respir Care. 2016. PMID: 27118876
-
Adherence to positive airway pressure therapy in adults and children.Curr Opin Pulm Med. 2009 Nov;15(6):585-90. doi: 10.1097/MCP.0b013e3283319b3f. Curr Opin Pulm Med. 2009. PMID: 19713846 Review.
-
The Effect of Patient-Facing Applications on Positive Airway Pressure Therapy Adherence: A Systematic Review.J Clin Sleep Med. 2019 May 15;15(5):769-777. doi: 10.5664/jcsm.7772. J Clin Sleep Med. 2019. PMID: 31053207 Free PMC article.
Cited by
-
Obstructive sleep apnea treatment and dementia risk in older adults.Sleep. 2021 Sep 13;44(9):zsab076. doi: 10.1093/sleep/zsab076. Sleep. 2021. PMID: 33769542 Free PMC article.
-
Effects of combined morbid insomnia and sleep apnea on long-term cardiovascular risk and all-cause mortality in elderly patients: a prospective cohort study.BMC Geriatr. 2024 Jul 21;24(1):622. doi: 10.1186/s12877-024-05147-2. BMC Geriatr. 2024. PMID: 39034410 Free PMC article.
-
The Present and Future of the Clinical Use of Physiological Traits for the Treatment of Patients with OSA: A Narrative Review.J Clin Med. 2024 Mar 13;13(6):1636. doi: 10.3390/jcm13061636. J Clin Med. 2024. PMID: 38541862 Free PMC article. Review.
-
Hospital screening for obstructive sleep apnea in patients admitted to a rural, tertiary care academic hospital with heart failure.Hosp Pract (1995). 2020 Dec;48(5):266-271. doi: 10.1080/21548331.2020.1799601. Epub 2020 Aug 4. Hosp Pract (1995). 2020. PMID: 32715796 Free PMC article.
-
Sleep and Breathing Conference highlights 2023: a summary by ERS Assembly 4.Breathe (Sheff). 2023 Sep;19(3):230168. doi: 10.1183/20734735.0168-2023. Epub 2023 Nov 14. Breathe (Sheff). 2023. PMID: 38020339 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
