

Displaced Myonuclei in Cancer Cachexia Suggest Altered Innervation
- PMID: 32041358
- PMCID: PMC7038037
- DOI: 10.3390/ijms21031092
Displaced Myonuclei in Cancer Cachexia Suggest Altered Innervation
Abstract
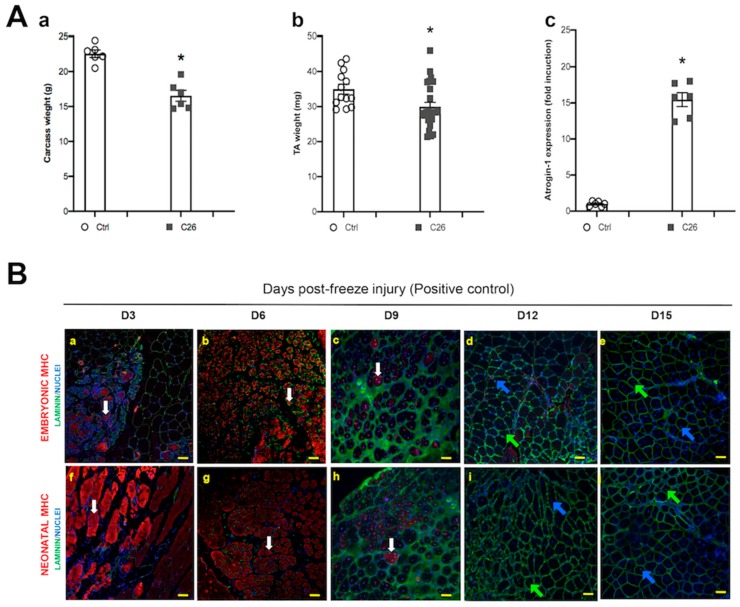
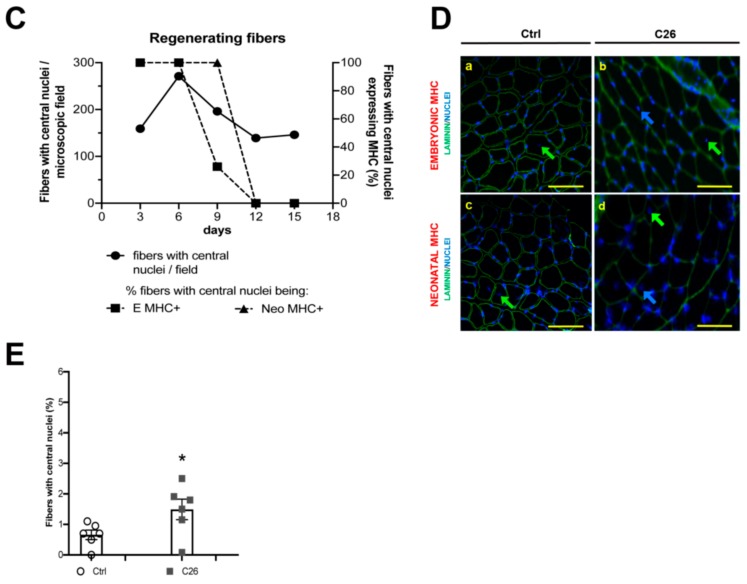
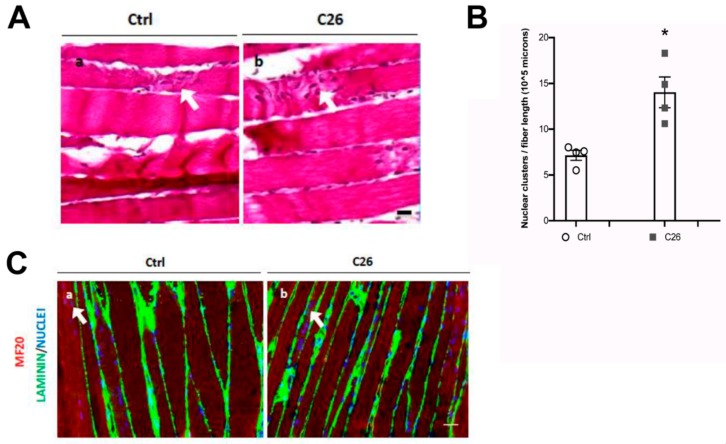
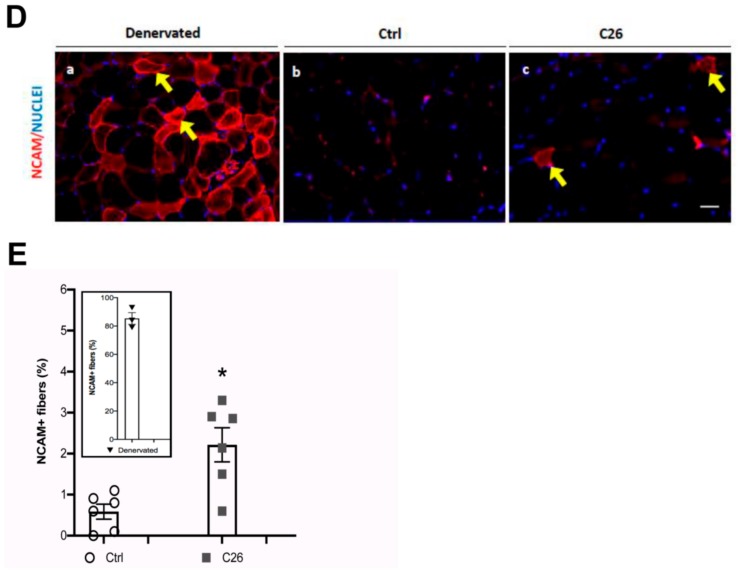
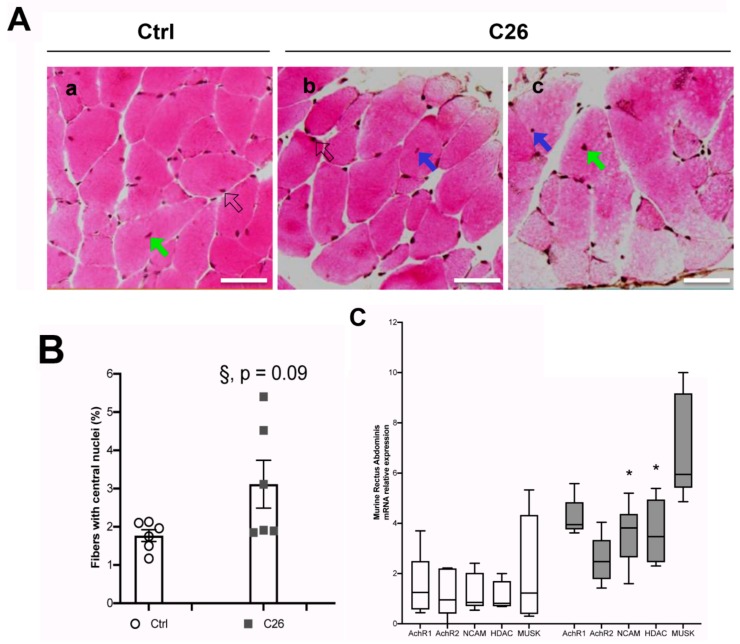
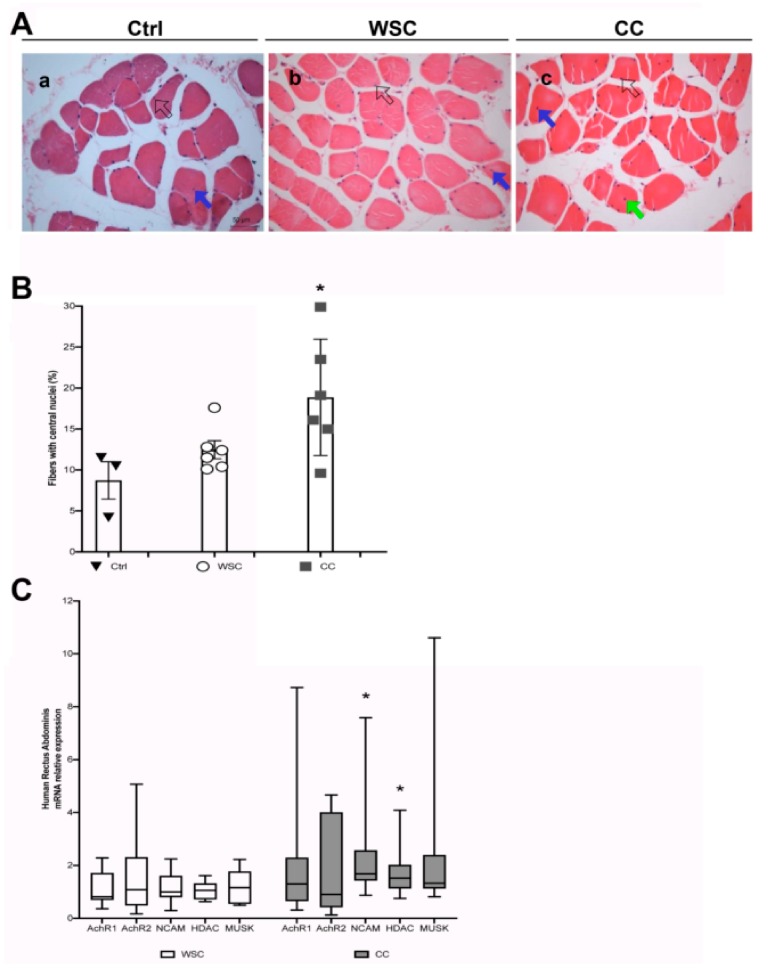
An idiopathic myopathy characterized by central nuclei in muscle fibers, a hallmark of muscle regeneration, has been observed in cancer patients. In cancer cachexia skeletal muscle is incapable of regeneration, consequently, this observation remains unaccounted for. In C26-tumor bearing, cachectic mice, we observed muscle fibers with central nuclei in the absence of molecular markers of bona fide regeneration. These clustered, non-peripheral nuclei were present in NCAM-expressing muscle fibers. Since NCAM expression is upregulated in denervated myofibers, we searched for additional makers of denervation, including AchRs, MUSK, and HDAC. This last one being also consistently upregulated in cachectic muscles, correlated with an increase of central myonuclei. This held true in the musculature of patients suffering from gastrointestinal cancer, where a progressive increase in the number of central myonuclei was observed in weight stable and in cachectic patients, compared to healthy subjects. Based on all of the above, the presence of central myonuclei in cancer patients and animal models of cachexia is consistent with motor neuron loss or NMJ perturbation and could underlie a previously neglected phenomenon of denervation, rather than representing myofiber damage and regeneration in cachexia. Similarly to aging, denervation-dependent myofiber atrophy could contribute to muscle wasting in cancer cachexia.
Keywords: Central nuclei; altered innervation; c26-colon carcinoma; cancer cachexia; muscle regeneration; striated muscles.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Valproic acid attenuates skeletal muscle wasting by inhibiting C/EBPβ-regulated atrogin1 expression in cancer cachexia.Am J Physiol Cell Physiol. 2016 Jul 1;311(1):C101-15. doi: 10.1152/ajpcell.00344.2015. Epub 2016 Apr 27. Am J Physiol Cell Physiol. 2016. PMID: 27122162
-
Cachexia does not induce loss of myonuclei or muscle fibres during xenografted prostate cancer in mice.Acta Physiol (Oxf). 2019 Mar;225(3):e13204. doi: 10.1111/apha.13204. Epub 2018 Nov 16. Acta Physiol (Oxf). 2019. PMID: 30325108
-
Molecular, cellular and physiological characterization of the cancer cachexia-inducing C26 colon carcinoma in mouse.BMC Cancer. 2010 Jul 8;10:363. doi: 10.1186/1471-2407-10-363. BMC Cancer. 2010. PMID: 20615237 Free PMC article.
-
Impaired regeneration: A role for the muscle microenvironment in cancer cachexia.Semin Cell Dev Biol. 2016 Jun;54:82-91. doi: 10.1016/j.semcdb.2015.09.009. Epub 2015 Sep 16. Semin Cell Dev Biol. 2016. PMID: 26385617 Free PMC article. Review.
-
Skeletal muscle regeneration in cancer cachexia.Clin Exp Pharmacol Physiol. 2016 May;43(5):522-7. doi: 10.1111/1440-1681.12559. Clin Exp Pharmacol Physiol. 2016. PMID: 26857538 Review.
Cited by
-
Exercise-mediated reinnervation of skeletal muscle in elderly people: An update.Eur J Transl Myol. 2022 Feb 28;32(1):10416. doi: 10.4081/ejtm.2022.10416. Eur J Transl Myol. 2022. PMID: 35234025 Free PMC article.
-
Progressive development of melanoma-induced cachexia differentially impacts organ systems in mice.Cell Rep. 2023 Jan 31;42(1):111934. doi: 10.1016/j.celrep.2022.111934. Epub 2022 Dec 29. Cell Rep. 2023. PMID: 36640353 Free PMC article.
-
Inflammation and Wasting of Skeletal Muscles in Kras-p53-Mutant Mice with Intraepithelial Neoplasia and Pancreatic Cancer-When Does Cachexia Start?Cells. 2022 May 11;11(10):1607. doi: 10.3390/cells11101607. Cells. 2022. PMID: 35626644 Free PMC article.
-
Vemurafenib improves muscle histopathology in a mouse model of LAMA2-related congenital muscular dystrophy.Dis Model Mech. 2023 Jun 1;16(6):dmm049916. doi: 10.1242/dmm.049916. Epub 2023 May 10. Dis Model Mech. 2023. PMID: 37021539 Free PMC article.
-
Age, cancer, and the dual burden of cancer and doxorubicin in skeletal muscle wasting in female rats: which one to blame?Biogerontology. 2025 Jan 24;26(1):47. doi: 10.1007/s10522-024-10182-y. Biogerontology. 2025. PMID: 39853446
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
