

Sentinel Lymph Node Biopsy in Head and Neck Melanoma: Long-term Outcomes, Prognostic Value, Accuracy, and Safety
- PMID: 32041486
- PMCID: PMC8012010
- DOI: 10.1177/0194599819899934
Sentinel Lymph Node Biopsy in Head and Neck Melanoma: Long-term Outcomes, Prognostic Value, Accuracy, and Safety
Abstract
Objective: To evaluate the long-term outcomes of sentinel lymph node biopsy (SLNB) for head and neck cutaneous melanoma (HNCM).
Study design: Retrospective cohort study.
Setting: Tertiary academic medical center.
Subjects and methods: Longitudinal review of a 356-patient cohort with HNCM undergoing SLNB from 1997 to 2007.
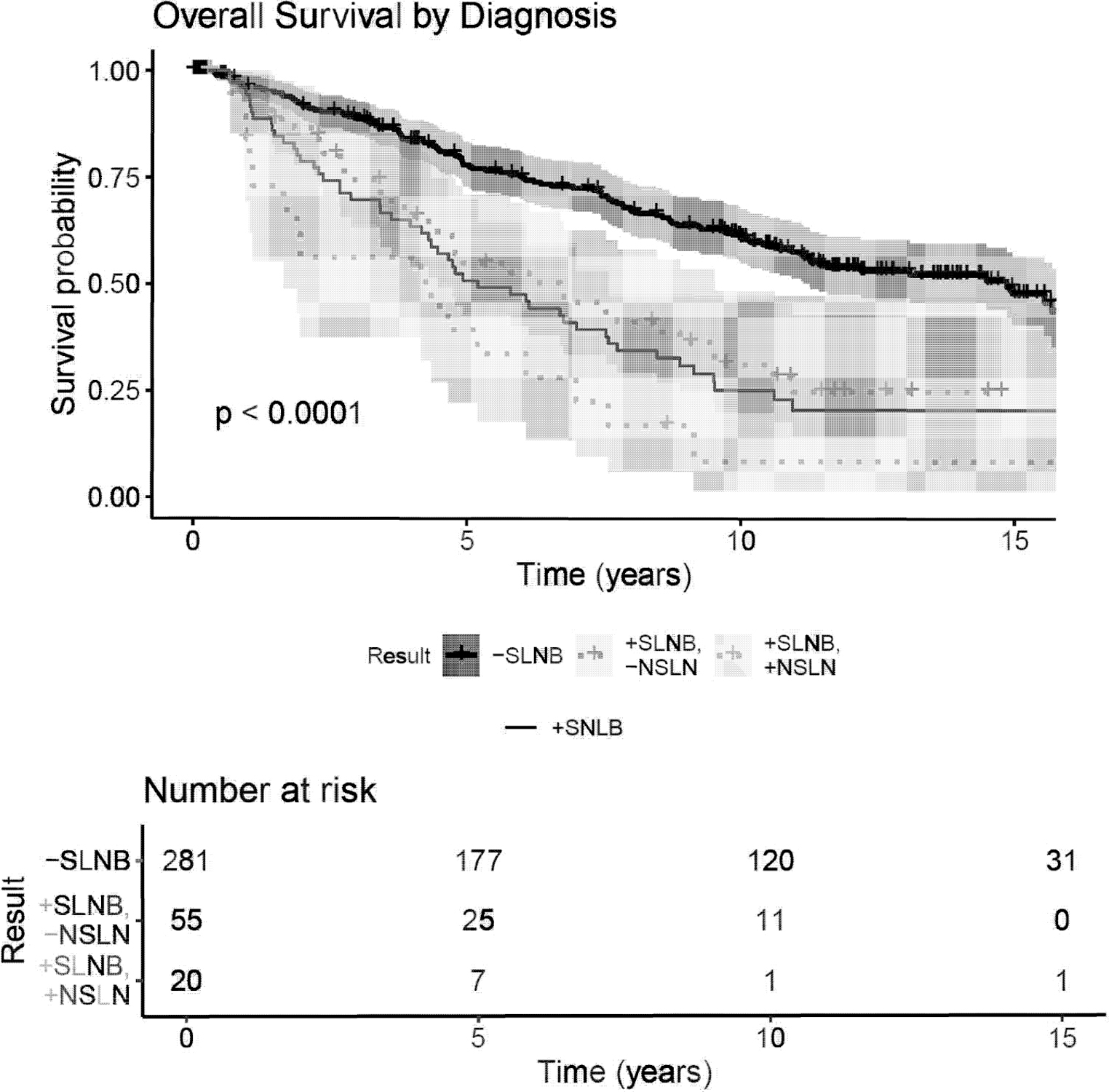
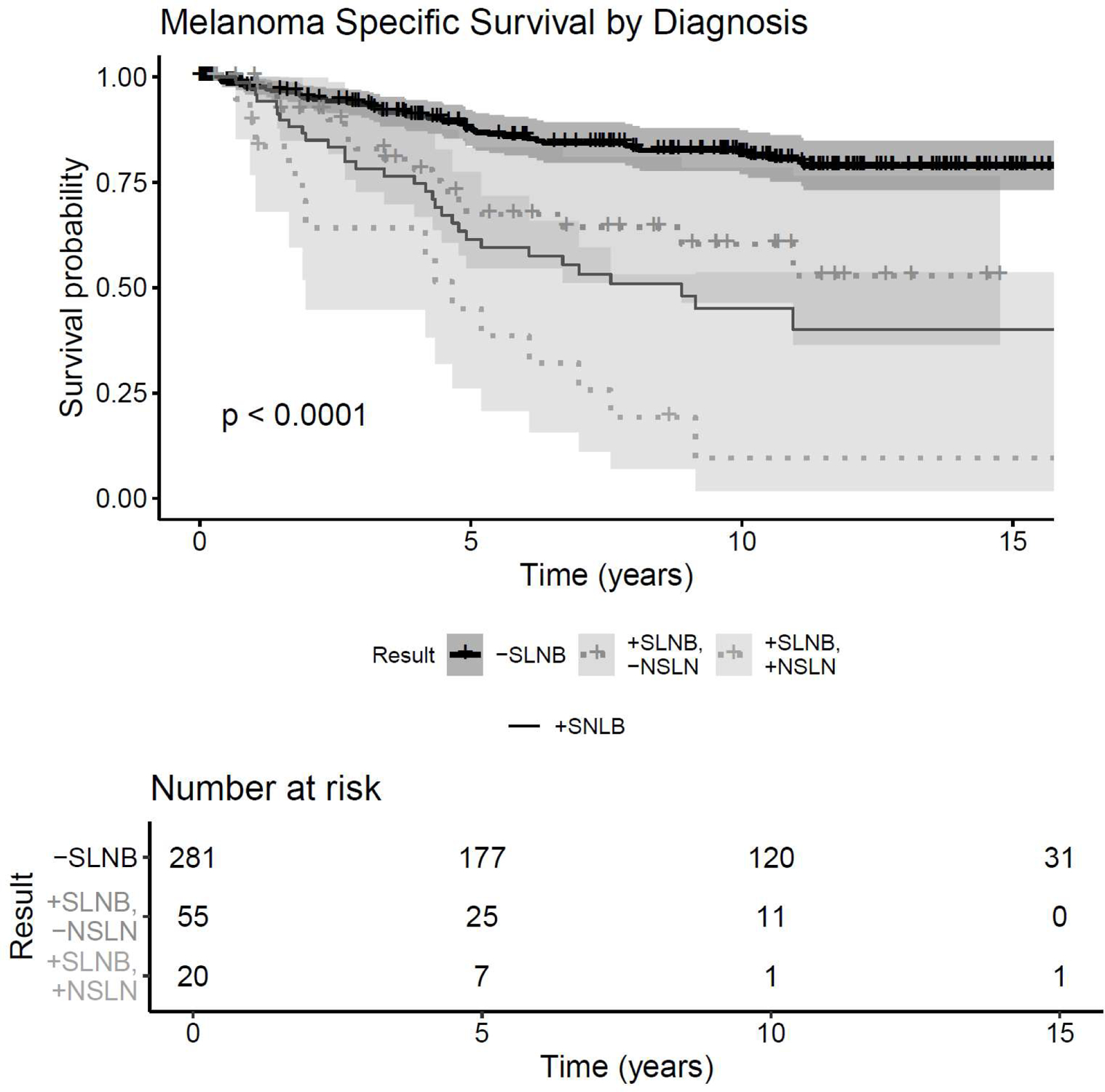
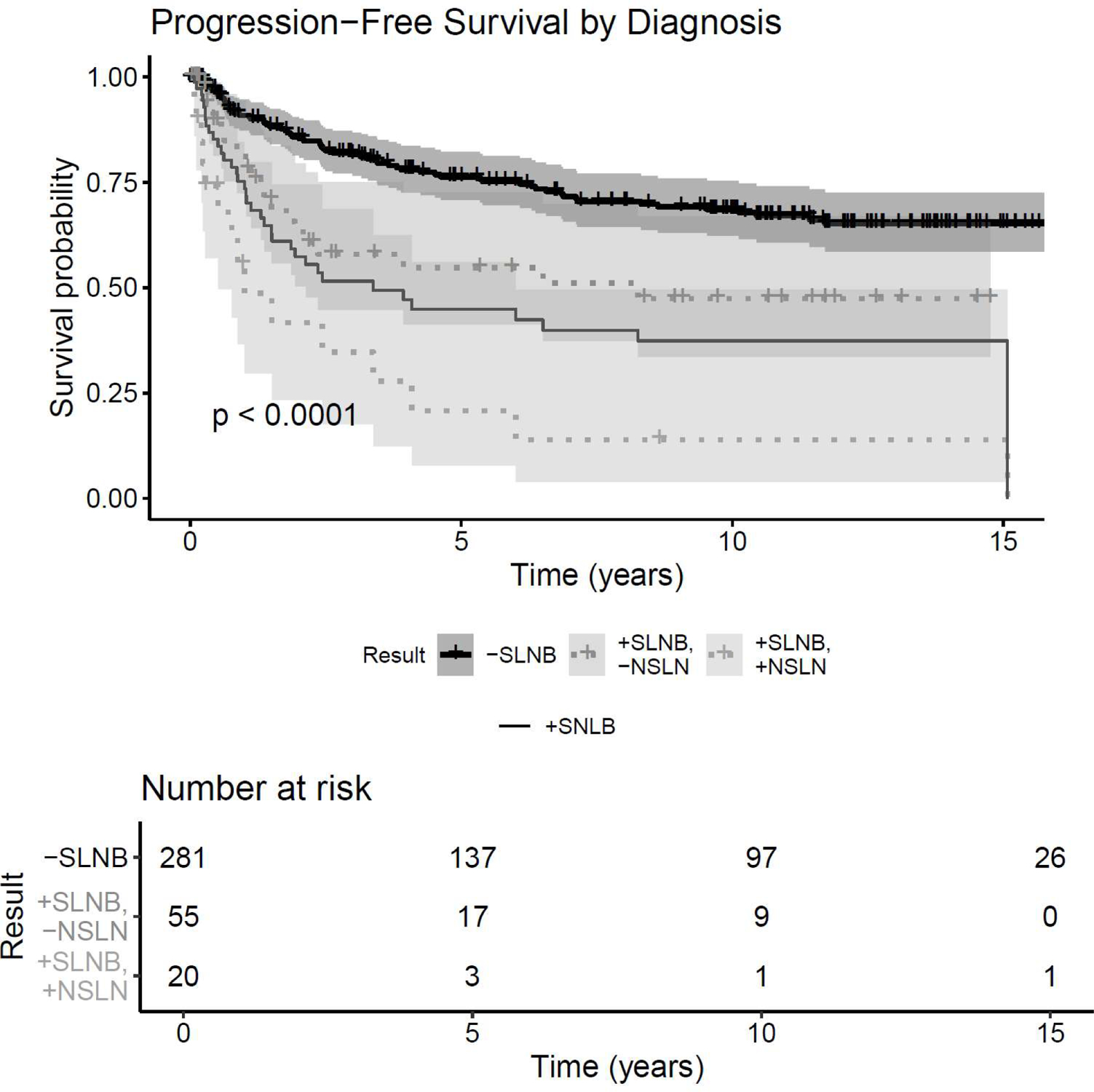
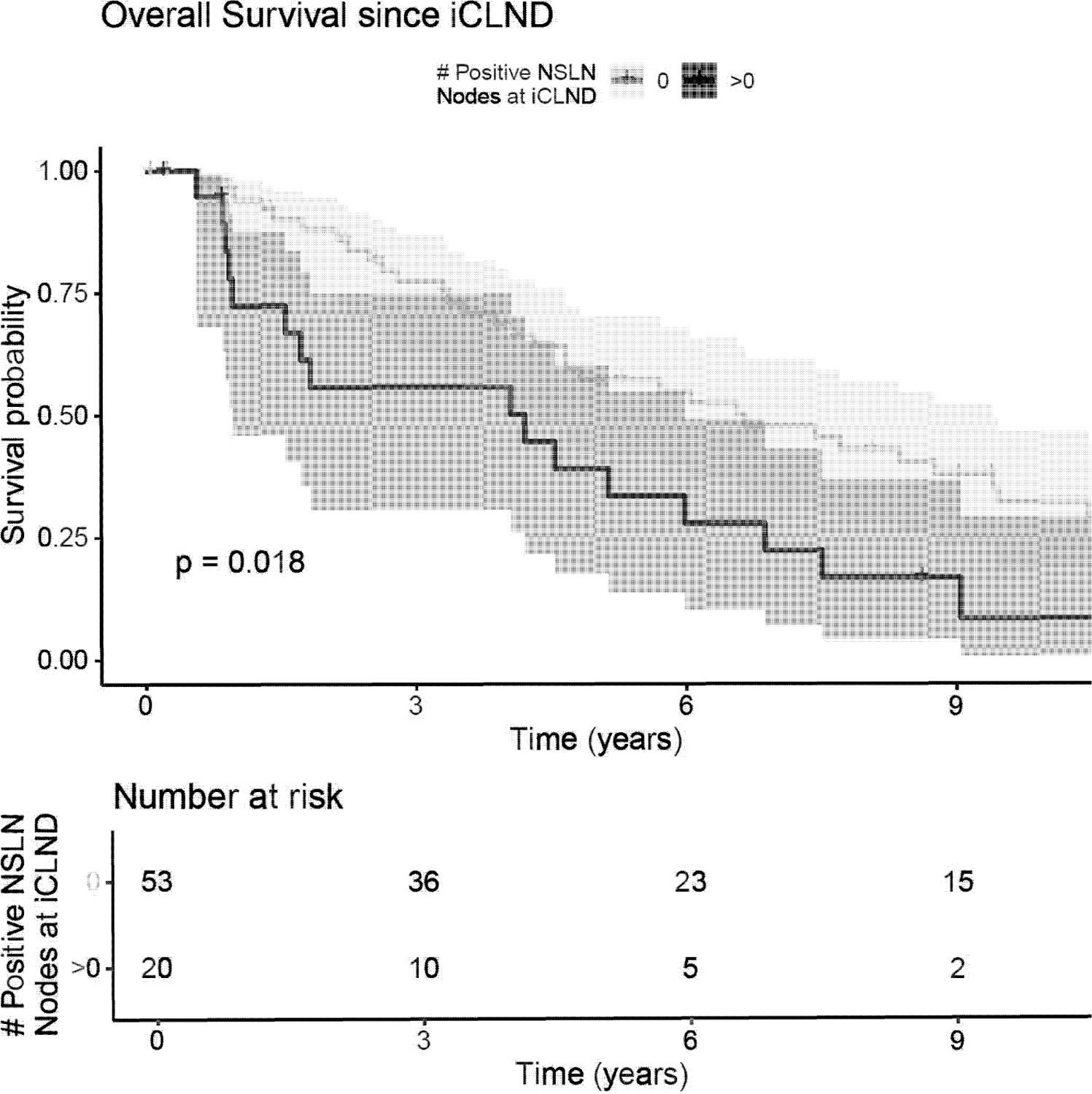
Results: Descriptive characteristics included the following: age, 53.5 ± 19 years (mean ± SD); sex, 26.8% female; median follow-up, 4.9 years; and Breslow depth, 2.52 ± 1.87 mm. Overall, 75 (21.1%) patients had a positive SLNB. Among patients undergoing completion lymph node dissection following positive SLNB, 20 (27.4%) had at least 1 additional positive nonsentinel lymph node. Eighteen patients with local control and negative SLNB developed regional disease, indicating a false omission rate of 6.4%, including 10 recurrences in previously unsampled basins. Ten-year overall survival (OS) and melanoma-specific survival (MSS) were significantly greater in the negative sentinel lymph node (SLN) cohort (OS, 61% [95% CI, 0.549-0.677]; MSS, 81.9% [95% CI, 0.769-0.873]) than the positive SLN cohort (OS, 31% [95% CI, 0.162-0.677]; MSS, 60.3% [95% CI, 0.464-0.785]) and positive SLN/positive nonsentinel lymph node cohort (OS, 8.4% [95% CI, 0.015-0.474]; MSS, 9.6% [95% CI, 0.017-0.536]). OS was significantly associated with SLN positivity (hazard ratio [HR], 2.39; P < .01), immunosuppression (HR, 2.37; P < .01), angiolymphatic invasion (HR, 1.91; P < .01), and ulceration (HR, 1.86; P < .01). SLN positivity (HR, 3.13; P < .01), angiolymphatic invasion (HR, 3.19; P < .01), and number of mitoses (P = .0002) were significantly associated with MSS. Immunosuppression (HR, 3.01; P < .01) and SLN status (HR, 2.84; P < .01) were associated with recurrence-free survival, and immunosuppression was the only factor significantly associated with regional recurrence (HR, 6.59; P < .01).
Conclusions: Long-term follow up indicates that SLNB showcases durable accuracy, safety, and prognostic importance for cutaneous HNCM.
Keywords: cutaneous; false omission; head and neck; melanoma; otolaryngology; sentinel lymph node biopsy.
Conflict of interest statement
Figures
Similar articles
-
Association of Complex Lymphatic Drainage in Head and Neck Cutaneous Melanoma With Sentinel Lymph Node Biopsy Outcomes: A Cohort Study and Literature Review.JAMA Otolaryngol Head Neck Surg. 2023 May 1;149(5):416-423. doi: 10.1001/jamaoto.2023.0076. JAMA Otolaryngol Head Neck Surg. 2023. PMID: 36892824 Free PMC article. Review.
-
Sentinel lymph node biopsy is accurate and prognostic in head and neck melanoma.Cancer. 2012 Feb 15;118(4):1040-7. doi: 10.1002/cncr.26288. Epub 2011 Jul 19. Cancer. 2012. PMID: 21773971
-
Cervical sentinel lymph node biopsy for melanomas of the head and neck and upper thorax.Arch Otolaryngol Head Neck Surg. 2000 Mar;126(3):313-21. doi: 10.1001/archotol.126.3.313. Arch Otolaryngol Head Neck Surg. 2000. PMID: 10722003
-
Accuracy and prognostic value of sentinel lymph node biopsy in head and neck melanomas.J Surg Res. 2014 Apr;187(2):518-24. doi: 10.1016/j.jss.2013.10.037. Epub 2013 Oct 23. J Surg Res. 2014. PMID: 24252855
-
Sentinel lymph node biopsy for melanoma: indications and rationale.Cancer Control. 2009 Jul;16(3):234-9. doi: 10.1177/107327480901600305. Cancer Control. 2009. PMID: 19556963 Review.
Cited by
-
Do Oncologic Outcomes From Head and Neck Versus Truncal and Extremity Melanoma Differ? A Single-Institution Single-Subspecialty Experience.Am Surg. 2022 Mar;88(3):480-488. doi: 10.1177/00031348211050813. Epub 2021 Nov 11. Am Surg. 2022. PMID: 34761683 Free PMC article.
-
False-negative sentinel lymph node biopsy for melanoma: a single-surgeon experience.Can J Surg. 2024 Sep 27;67(5):E337-E344. doi: 10.1503/cjs.016023. Print 2024 Sep-Oct. Can J Surg. 2024. PMID: 39332833 Free PMC article.
References
-
- Morton DL, Wen DR, Wong JH, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg. 1992;127(4):392–399. - PubMed
-
- Morton DL, Thompson JF, Cochran AJ, et al. Sentinel-node biopsy or nodal observation in melanoma. N Engl J Med. 2006;355(13):1307–1317. - PubMed
-
- Schmalbach CE, Bradford CR. Is sentinel lymph node biopsy the standard of care for cutaneous head and neck melanoma? laryngoscope. 2015;125(1):153–160. - PubMed
-
- McMasters KM, Reintgen DS, Ross Ml, et al. Sentinel lymph node biopsy for melanoma: how many radioactive nodes should be removed? Ann Surg Oncol. 2001;8(3):192–197. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
