

Risk factors for pneumonia and influenza hospitalizations in long-term care facility residents: a retrospective cohort study
- PMID: 32041538
- PMCID: PMC7011520
- DOI: 10.1186/s12877-020-1457-8
Risk factors for pneumonia and influenza hospitalizations in long-term care facility residents: a retrospective cohort study
Abstract
Background: Older adults who reside in long-term care facilities (LTCFs) are at particularly high risk for infection, morbidity and mortality from pneumonia and influenza (P&I) compared to individuals of younger age and those living outside institutional settings. The risk factors for P&I hospitalizations that are specific to LTCFs remain poorly understood. Our objective was to evaluate the incidence of P&I hospitalization and associated person- and facility-level factors among post-acute (short-stay) and long-term (long-stay) care residents residing in LTCFs from 2013 to 2015.
Methods: In this retrospective cohort study, we used Medicare administrative claims linked to Minimum Data Set and LTCF-level data to identify short-stay (< 100 days, index = admission date) and long-stay (100+ days, index = day 100) residents who were followed from the index date until the first of hospitalization, LTCF discharge, Medicare disenrollment, or death. We measured incidence rates (IRs) for P&I hospitalization per 100,000 person-days, and estimated associations with baseline demographics, geriatric syndromes, clinical characteristics, and medication use using Cox regression models.
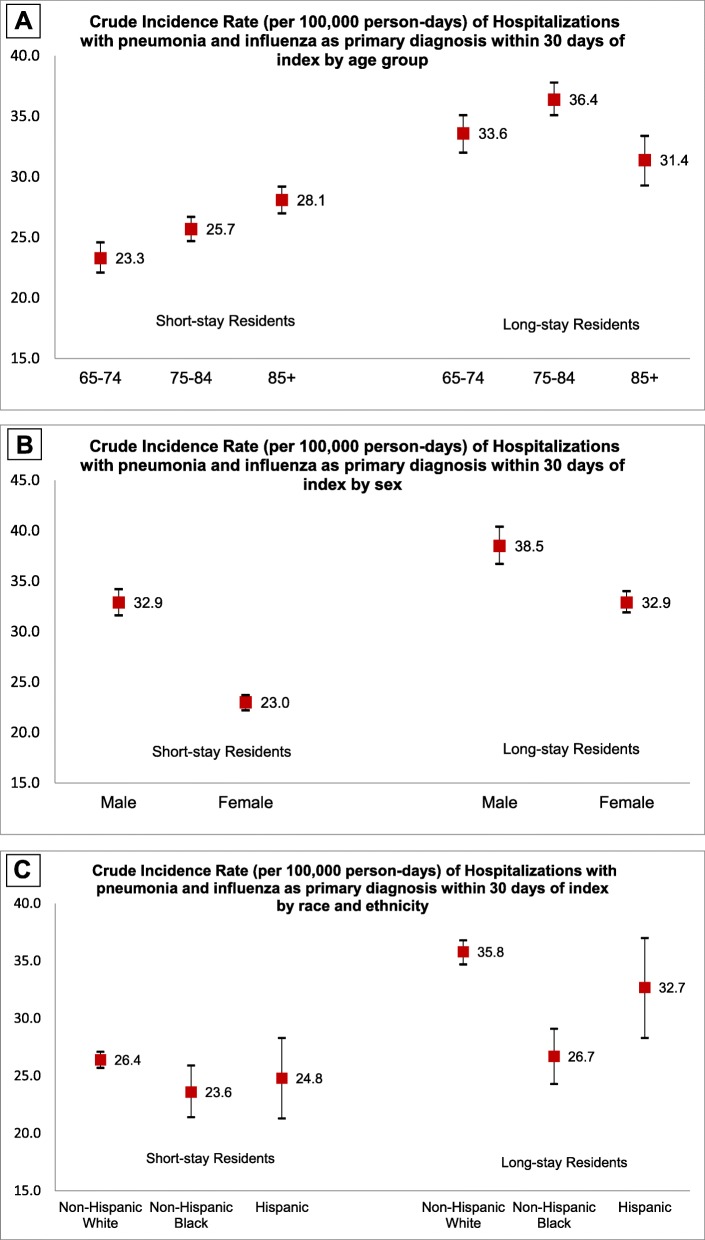
Results: We analyzed data from 1,118,054 short-stay and 593,443 long-stay residents. The crude 30-day IRs (95% CI) of hospitalizations with P&I in the principal position were 26.0 (25.4, 26.6) and 34.5 (33.6, 35.4) among short- and long-stay residents, respectively. The variables associated with P&I varied between short and long-stay residents, and common risk factors included: advanced age (85+ years), admission from an acute hospital, select cardiovascular and respiratory conditions, impaired functional status, and receipt of antibiotics or Beers criteria medications. Facility staffing and care quality measures were important risk factors among long-stay residents but not in short-stay residents.
Conclusions: Short-stay residents had lower crude 30- and 90-day incidence rates of P&I hospitalizations than long-stay LTCF residents. Differences in risk factors for P&I between short- and long-stay populations suggest the importance of considering distinct profiles of post-acute and long-term care residents in infection prevention and control strategies in LTCFs. These findings can help clinicians target interventions to subgroups of LTCF residents at highest P&I risk.
Keywords: Influenza; Long-term care; Medicare; Nursing homes; Pneumonia.
Conflict of interest statement
EB, ARZ, KWM, and PM declare no conflicts of interest. RVA and AC are employed by Sanofi Pasteur. SG reports grants and personal fees from Seqirus, Sanofi; and consulting or speaker fees from Sanofi, Merck, Longeveron, and the Gerontological Society of America for research related to vaccines or nursing home care quality.
Figures
Comment in
-
Pneumonie und Influenza: Diese Pflegepatienten landen in der Klinik : Infektionen -- Autor: H. J. Heppner.MMW Fortschr Med. 2020 Oct;162(17):25. doi: 10.1007/s15006-020-4428-2. MMW Fortschr Med. 2020. PMID: 33020859 Review. German. No abstract available.
References
-
- Bradley S. Strategies to improve outcomes in nursing home residents with modifiable risk factors for respiratory tract infections. Pa Patient Saf Advis. 2011;8(4):131–137.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
