

Six years' experience with LipidSeq: clinical and research learnings from a hybrid, targeted sequencing panel for dyslipidemias
- PMID: 32041611
- PMCID: PMC7011550
- DOI: 10.1186/s12920-020-0669-2
Six years' experience with LipidSeq: clinical and research learnings from a hybrid, targeted sequencing panel for dyslipidemias
Abstract
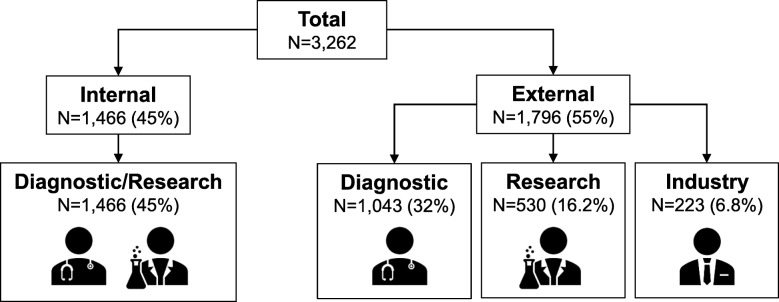
Background: In 2013, our laboratory designed a targeted sequencing panel, "LipidSeq", to study the genetic determinants of dyslipidemia and metabolic disorders. Over the last 6 years, we have analyzed 3262 patient samples obtained from our own Lipid Genetics Clinic and international colleagues. Here, we highlight our findings and discuss research benefits and clinical implications of our panel.
Methods: LipidSeq targets 69 genes and 185 single-nucleotide polymorphisms (SNPs) either causally related or associated with dyslipidemia and metabolic disorders. This design allows us to simultaneously evaluate monogenic-caused by rare single-nucleotide variants (SNVs) or copy-number variants (CNVs)-and polygenic forms of dyslipidemia. Polygenic determinants were assessed using three polygenic scores, one each for low-density lipoprotein cholesterol, triglyceride, and high-density lipoprotein cholesterol.
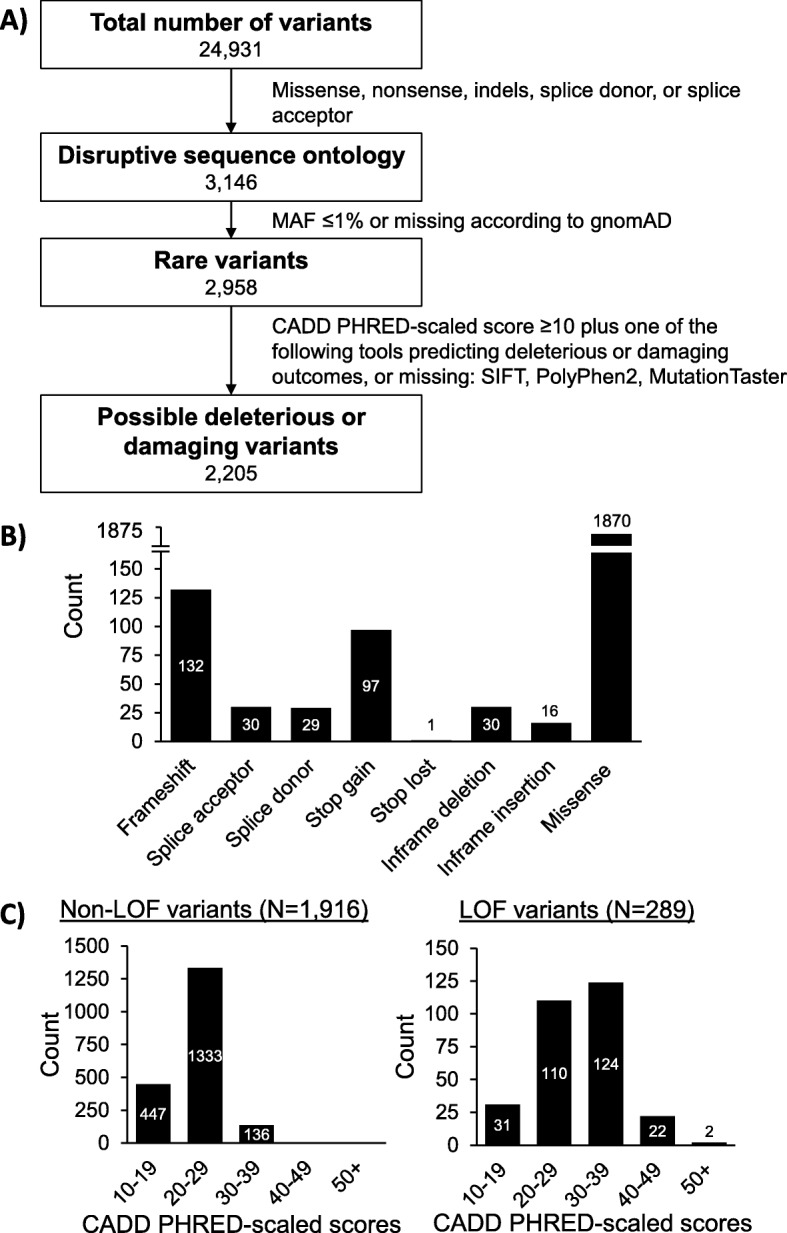
Results: Among 3262 patient samples evaluated, the majority had hypertriglyceridemia (40.1%) and familial hypercholesterolemia (28.3%). Across all samples, we identified 24,931 unique SNVs, including 2205 rare variants predicted disruptive to protein function, and 77 unique CNVs. Considering our own 1466 clinic patients, LipidSeq results have helped in diagnosis and improving treatment options.
Conclusions: Our LipidSeq design based on ontology of lipid disorders has enabled robust detection of variants underlying monogenic and polygenic dyslipidemias. In more than 50 publications related to LipidSeq, we have described novel variants, the polygenic nature of many dyslipidemias-some previously thought to be primarily monogenic-and have uncovered novel mechanisms of disease. We further demonstrate several tangible clinical benefits of its use.
Keywords: Dyslipidemia; Familial hypercholesterolemia; Hypertriglyceridemia; Lipid; Lipoprotein; Metabolic disorder; Targeted next-generation sequencing panel.
Conflict of interest statement
R.A.H. reports consulting fees from Acasti, Aegerion, Akcea/Ionis, Amgen and Sanofi. The other authors have no disclosures.
Figures


References
-
- Hegele RA, Ginsberg HN, Chapman MJ, Nordestgaard BG, Kuivenhoven JA, Averna M, Boren J, Bruckert E, Catapano AL, Descamps OS, et al. The polygenic nature of hypertriglyceridaemia: implications for definition, diagnosis, and management. Lancet Diabetes Endocrinol. 2014;2(8):655–666. doi: 10.1016/S2213-8587(13)70191-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
