

Pre-operative sera interleukin-6 in the diagnosis of high-grade serous ovarian cancer
- PMID: 32042020
- PMCID: PMC7010756
- DOI: 10.1038/s41598-020-59009-z
Pre-operative sera interleukin-6 in the diagnosis of high-grade serous ovarian cancer
Abstract
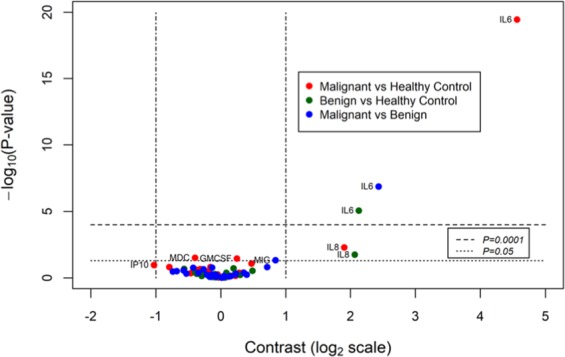
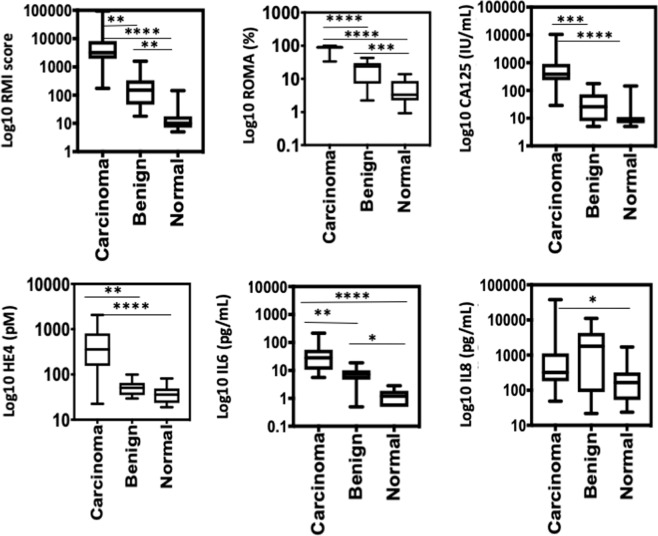
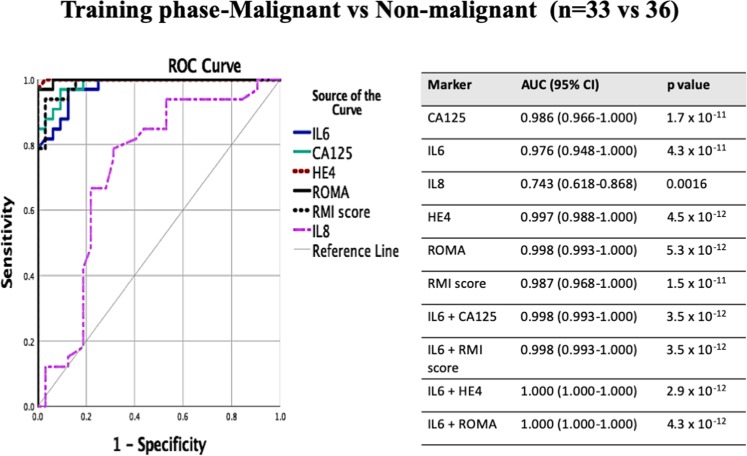
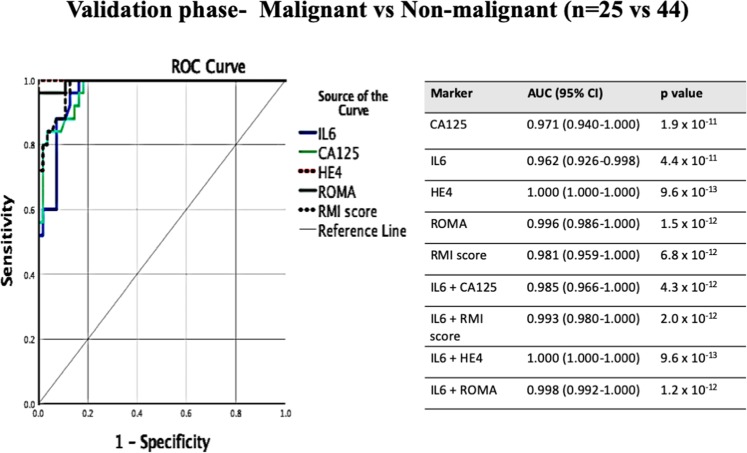
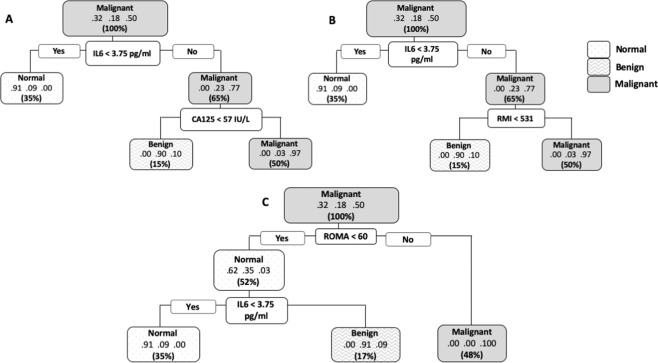
Pre-operative discrimination of malignant masses is crucial for accurate diagnosis and prompt referral to a gynae oncology centre for optimal surgical intervention. HGSOC progression is correlated with local and systemic inflammation. We hypothesised that inclusion of inflammatory biomarkers in sera may improve diagnostic tests. In the training cohort, we tested four existing clinical tests (RMI score and ROMA, CA125 and HE4) and a panel of 28 immune soluble biomarkers in sera from 66 patients undergoing surgery for suspected ovarian cancer. Six promising immune biomarkers alone, or in combination with conventional tests, were subsequently analysed in an independent validation cohort (n = 69). IL-6 was identified as the main driver of variability followed closely by conventional diagnostic tests. Median sera IL-6 was higher in HGSOC patients compared to those with a benign mass or controls with normal ovaries (28.3 vs 7.3 vs 1.2 pg/ml, p < 0.0001). The combination of IL-6 further improved the overall predictive probability of the conventional tests. Modelling a two-step triage of women with a suspicious ovarian mass, with IL-6 > 3.75 pg/ml as primary triage followed by conventional tests (CA125 or RMI score) identified ovarian cancer in patients with a misclassification rate of 4.54-3.03%, superior to the use of CA125 or RMI alone (9.09 to 10.60). The validation cohort demonstrated a similar improvement in the diagnostic sensitivity following addition of IL-6. IL-6 in combination with conventional tests may be a useful clinical biomarker for triage of patients with a suspected malignant ovarian mass.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Diagnostic accuracy of CA125 and HE4 in ovarian carcinoma patients and the effect of confounders on their serum levels.Curr Probl Cancer. 2019 Oct;43(5):450-460. doi: 10.1016/j.currproblcancer.2018.12.004. Epub 2019 Jan 16. Curr Probl Cancer. 2019. PMID: 30670303
-
A multiplex biomarker assay improves the diagnostic performance of HE4 and CA125 in ovarian tumor patients.PLoS One. 2020 Oct 19;15(10):e0240418. doi: 10.1371/journal.pone.0240418. eCollection 2020. PLoS One. 2020. PMID: 33075095 Free PMC article.
-
HE4, CA125, the Risk of Malignancy Algorithm and the Risk of Malignancy Index and complex pelvic masses - a prospective comparison in the pre-operative evaluation of pelvic masses in an Australian population.Aust N Z J Obstet Gynaecol. 2015 Oct;55(5):493-7. doi: 10.1111/ajo.12363. Epub 2015 Jul 14. Aust N Z J Obstet Gynaecol. 2015. PMID: 26172511
-
[Diagnostic and prognostic value of tumor markers, scores (clinical and biological) algorithms, in front of an ovarian mass suspected of an epithelial ovarian cancer: Article drafted from the French Guidelines in oncology entitled "Initial management of patients with epithelial ovarian cancer" developed by FRANCOGYN, CNGOF, SFOG, GINECO-ARCAGY under the aegis of CNGOF and endorsed by INCa].Gynecol Obstet Fertil Senol. 2019 Feb;47(2):134-154. doi: 10.1016/j.gofs.2018.12.013. Epub 2019 Feb 5. Gynecol Obstet Fertil Senol. 2019. PMID: 30733191 Review. French.
-
HE4 in the differential diagnosis of ovarian masses.Clin Chim Acta. 2015 Jun 15;446:147-55. doi: 10.1016/j.cca.2015.03.047. Epub 2015 Apr 16. Clin Chim Acta. 2015. PMID: 25892674 Review.
Cited by
-
Prognostic and Clinical Value of Interleukin 6 and CD45+CD14+ Inflammatory Cells with PD-L1+/PD-L2+ Expression in Patients with Different Manifestation of Ovarian Cancer.J Immunol Res. 2020 Sep 30;2020:1715064. doi: 10.1155/2020/1715064. eCollection 2020. J Immunol Res. 2020. PMID: 33062717 Free PMC article.
-
New Predictive Biomarkers for Ovarian Cancer.Diagnostics (Basel). 2021 Mar 7;11(3):465. doi: 10.3390/diagnostics11030465. Diagnostics (Basel). 2021. PMID: 33800113 Free PMC article. Review.
-
Two Biosensors for the Determination of Interleukin-6 in Blood Plasma by Array SPRi.Biosensors (Basel). 2022 Jun 14;12(6):412. doi: 10.3390/bios12060412. Biosensors (Basel). 2022. PMID: 35735559 Free PMC article.
-
Absolute Neutrophil Count and Mean Platelet Volume in the Blood as Biomarkers to Detect Lung Cancer.Dis Markers. 2020 Apr 21;2020:1371964. doi: 10.1155/2020/1371964. eCollection 2020. Dis Markers. 2020. PMID: 32377267 Free PMC article.
-
Mapping Epitopes Recognised by Autoantibodies Shows Potential for the Diagnosis of High-Grade Serous Ovarian Cancer and Monitoring Response to Therapy for This Malignancy.Cancers (Basel). 2021 Aug 20;13(16):4201. doi: 10.3390/cancers13164201. Cancers (Basel). 2021. PMID: 34439354 Free PMC article.
References
-
- Soslow RA. Histologic subtypes of ovarian carcinoma: an overview. International Journal of Gynecological Pathology. 2008;27:161–174. - PubMed
-
- Australian Institute of Health and Welfare & National Breast and Ovarian Cancer Centre (Australia). Ovarian cancer in Australia: an overview, 2010. Australian Institute of Health and Welfare: Canberra (2010).
-
- Sioulas VD, et al. Optimal primary management of bulky stage IIIC ovarian, fallopian tube and peritoneal carcinoma: Are the only options complete gross resection at primary debulking surgery or neoadjuvant chemotherapy? Gynecologic oncology. 2017;145:15–20. doi: 10.1016/j.ygyno.2017.02.023. - DOI - PMC - PubMed
-
- Kontoninas, Z. et al. Tumor Markers in Diagnosis and Follow up of Haematologic Malignancies. Am Soc Hematology (2016).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
