

Anterior Capsule Reconstruction of the Native Hip: A Technique Guide
- PMID: 32042580
- PMCID: PMC7000316
- DOI: 10.1016/j.eats.2019.06.014
Anterior Capsule Reconstruction of the Native Hip: A Technique Guide
Abstract
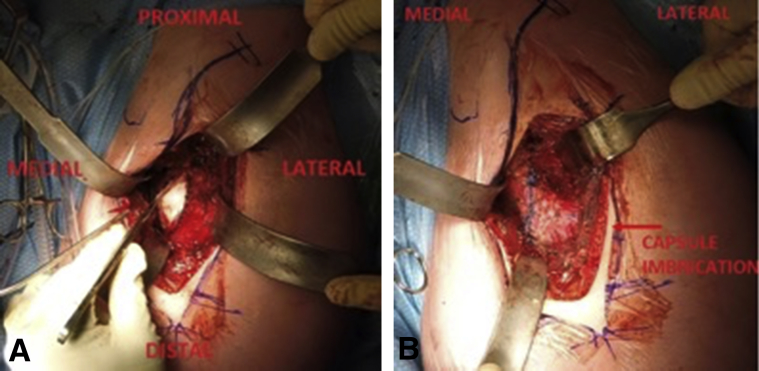
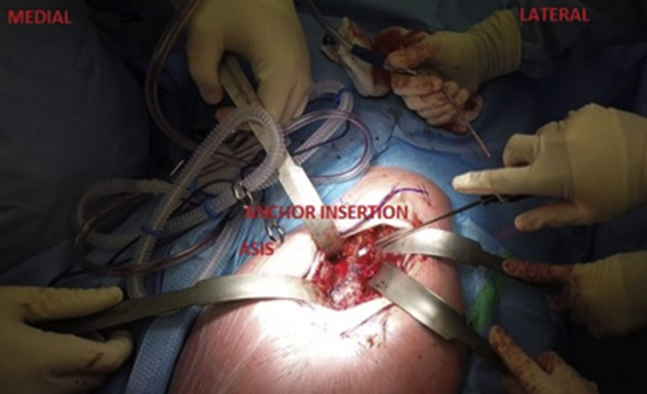
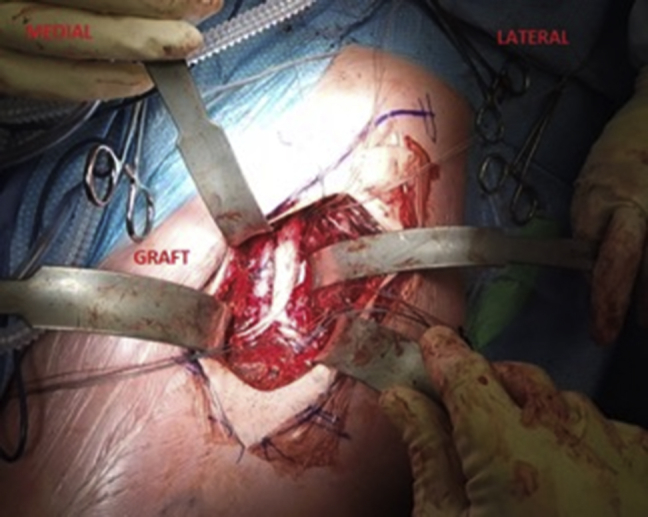
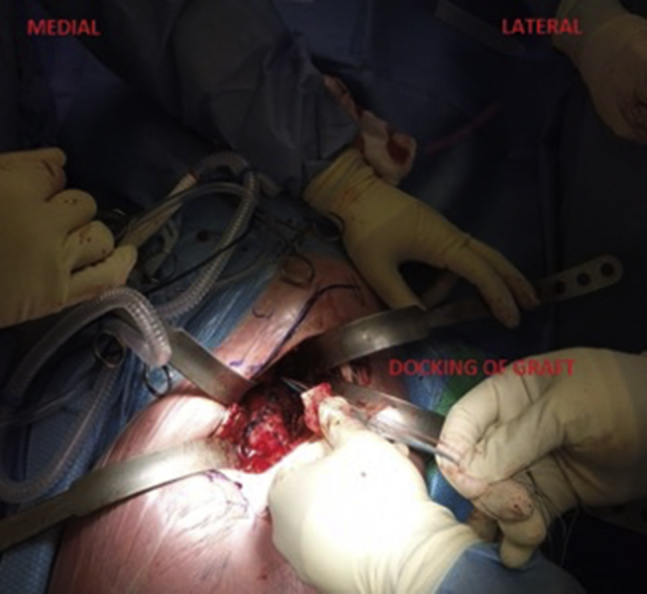
This is a technique guide for open anterior capsule reconstruction in unstable native hips due to Ehlers-Danlos syndrome. Ehlers-Danlos syndrome is a connective tissue disease that predisposes an individual to hypermobility of their soft tissues and recurrent subluxations and dislocations of their joints. This may lead to constant instability, guarding of the hip, and subsequent arthritic changes and poor quality of life. We demonstrate anterior capsule reconstruction of the hip using an Achilles tendon allograft performed through a direct anterior approach to the hip (Heuter's approach). This technique guide outlines in detail the surgical steps required to accomplish this reconstructive procedure. Furthermore, a narrated surgical video is provided that clearly depicts the anticipated result of the increased constrained provided to the hip from the anterior capsule reconstruction using an Achilles tendon allograft.
© 2019 by the Arthroscopy Association of North America. Published by Elsevier.
Figures




References
-
- Yeung M., Khan M., Williams D., Ayeni O.R. Anterior hip capsuloligamentous reconstruction with Achilles allograft following gross hip instability post-arthroscopy. Knee Surg Sports Traumatol Arthrosc. 2017;25:3–8. - PubMed
-
- Telleria J.J.M., Lindsey D.P., Giori N.J., Safran M.R. A quantitative assessment of the insertional footprints of the hip joint capsular ligaments and their spanning fibers for reconstruction. Clin Anat. 2014;27:489–497. - PubMed
-
- Larson C.M., Stone R.M., Grossi E.F., Giveans M.R., Cornelsen G.D. Ehlers-Danlos syndrome: Arthroscopic management for extreme soft-tissue hip instability. Arthroscopy. 2015;31:2287–2294. - PubMed
LinkOut - more resources
Full Text Sources
