

Using transperineal ultrasound to predict labor onset
- PMID: 32042734
- PMCID: PMC6990016
- DOI: 10.21037/atm.2019.12.11
Using transperineal ultrasound to predict labor onset
Abstract
Background: Accurate diagnosis of labor onset is especially important for the counseling about elective induction of labor. The study aimed to evaluate whether transperineal ultrasound could better predict the timing and likelihood of spontaneous labor at term.
Methods: This single-center study was conducted between 2018 and 2019.Data on singleton pregnant women after 39 weeks and before labor onset were retrospectively reviewed.
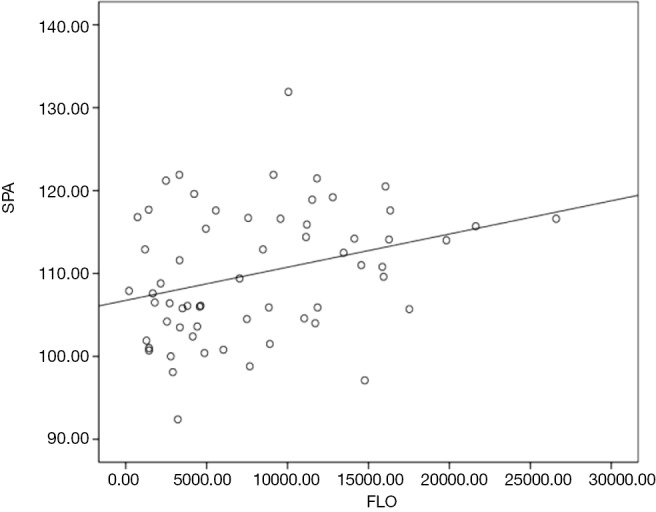
Results: All the transperineal ultrasound parameters were well reproducible between the two doctors [intraclass correlation coefficient (ICC) for progression distance(PD) was 0.892, P<0.001], [ICC for angle of progression (AoP) was 0.881, P<0.001], [ICC for subpubic arch angle (SPA) was 0.766, P<0.001], [ICC for width of symphysis pubis (WSP) was 0.803, P<0.001]. For the pregnant women before 40 weeks, the width of symphysis pubis changed gradually with the of spontaneous labor (WSP) (r=0.33, P<0.05). For all included women, the SPA correlated with the time of spontaneous labor (SPA) (r=0.31, P<0.05).
Conclusions: The antepartum transperineal ultrasound is a simple and objective technique that better observes the initiation of labor. And with the WSP and SPA we were able to predict labor onset and help in counseling about elective induction of labor.
Keywords: Labor onset; angle of progression (AoP); progression distance (PD); subpubic arch angle (SPA); width of symphysis pubis (WSP).
2019 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures







Comment in
-
Transperineal ultrasound to predict vaginal deliveries.Ann Transl Med. 2020 May;8(9):574. doi: 10.21037/atm-20-3144. Ann Transl Med. 2020. PMID: 32566601 Free PMC article. No abstract available.
Similar articles
-
Prediction of spontaneous vaginal delivery in nulliparous women with a prolonged second stage of labor: the value of intrapartum ultrasound.Am J Obstet Gynecol. 2019 Dec;221(6):642.e1-642.e13. doi: 10.1016/j.ajog.2019.09.045. Epub 2019 Oct 4. Am J Obstet Gynecol. 2019. PMID: 31589867
-
Correlation between Subpubic Arch Angle and Mode of Delivery in Large-for-Gestational-Age Fetuses.Fetal Diagn Ther. 2018;44(3):221-227. doi: 10.1159/000481169. Epub 2017 Dec 13. Fetal Diagn Ther. 2018. PMID: 29232667
-
Fetal head descent assessed by transabdominal ultrasound: a prospective observational study.Am J Obstet Gynecol. 2022 Jan;226(1):112.e1-112.e10. doi: 10.1016/j.ajog.2021.07.030. Epub 2021 Aug 10. Am J Obstet Gynecol. 2022. PMID: 34389293
-
Intrapartum ultrasound measurement of angle of progression at the onset of the second stage of labor for prediction of spontaneous vaginal delivery in term singleton pregnancies: a systematic review and meta-analysis.Am J Obstet Gynecol. 2022 Feb;226(2):205-214.e2. doi: 10.1016/j.ajog.2021.07.031. Epub 2021 Aug 9. Am J Obstet Gynecol. 2022. PMID: 34384775
-
The usefulness of ultrasound before induction of labor.Am J Obstet Gynecol MFM. 2021 Nov;3(6S):100423. doi: 10.1016/j.ajogmf.2021.100423. Epub 2021 Jun 12. Am J Obstet Gynecol MFM. 2021. PMID: 34129996 Review.
Cited by
-
Application of Predictive Analytics in Pregnancy, Birth, and Postpartum Nursing Care.MCN Am J Matern Child Nurs. 2025 Mar-Apr 01;50(2):66-77. doi: 10.1097/NMC.0000000000001082. Epub 2025 Feb 25. MCN Am J Matern Child Nurs. 2025. PMID: 39724545 Free PMC article.
-
Predicting labor onset relative to the estimated date of delivery using smart ring physiological data.NPJ Digit Med. 2023 Aug 19;6(1):153. doi: 10.1038/s41746-023-00902-y. NPJ Digit Med. 2023. PMID: 37598232 Free PMC article.
-
Transperineal ultrasound to predict vaginal deliveries.Ann Transl Med. 2020 May;8(9):574. doi: 10.21037/atm-20-3144. Ann Transl Med. 2020. PMID: 32566601 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources