

Traumatic macular hole study: a multicenter comparative study between immediate vitrectomy and six-month observation for spontaneous closure
- PMID: 32042742
- PMCID: PMC6989969
- DOI: 10.21037/atm.2019.12.20
Traumatic macular hole study: a multicenter comparative study between immediate vitrectomy and six-month observation for spontaneous closure
Abstract
Background: Closure of traumatic macular hole (TMH) can be achieved spontaneously or by surgical intervention. Thus far, there exist no prospective comparative studies that have analyzed the difference between the two modalities. This study aimed to compare the anatomical and visual recovery of eyes with TMH following either an immediate vitrectomy or six-month observation.
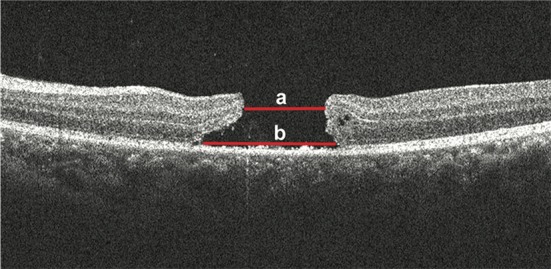
Methods: This was a multicenter prospective comparative study. Eight centers participated in the study. Patient data from 40 eyes with a recent history of blunt ocular trauma and newly formed full-thickness TMH were recruited in this study. The participating patients selected between an early vitrectomy or a six-month observation after a doctor explained the potential benefits and risks of both strategies in an unbiased manner. Twenty-five patients underwent an immediate vitrectomy, and 15 patients received six-month observation. Patients were assessed by spectral-domain optical coherence tomography (SD-OCT) and best-corrected visual acuity (BCVA).
Results: Closure rates were 66.7% for the observational group, and 100% for the surgical group (P=0.002). There were no vision-threatening ocular complications in both groups. For the observational group, the mean closure time was 2.5±1.6 months, and 80% of the hole closure occurred within 3 months; cystic edema on the edge of the hole at baseline was significantly more frequent in the non-closed subgroup than in the closed subgroup (P=0.03). There were no significant differences in the foveal microstructure and in the final visual outcome between the spontaneously closed cases and the surgically closed cases.
Conclusions: TMH had a moderately high incidence of spontaneous closure, but an immediate vitrectomy achieved an even higher closure rate. Vitrectomy was effective and safe to treat TMH, while a 3-month observation for spontaneous closure may be an alternative modality for TMH management. Cystic edema on the edge of the hole may be an unfavorable factor for the spontaneous closure of TMH.
Keywords: Traumatic macular hole (TMH); observation; vitrectomy.
2019 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures




Comment in
-
Traumatic macular holes: to operate, or not to operate, that is the question.Ann Transl Med. 2020 Aug;8(15):916. doi: 10.21037/atm.2020.04.50. Ann Transl Med. 2020. PMID: 32953716 Free PMC article. No abstract available.
Similar articles
-
Traumatic Macular Hole: Clinical Management and Optical Coherence Tomography Features.J Ophthalmol. 2020 Oct 20;2020:4819468. doi: 10.1155/2020/4819468. eCollection 2020. J Ophthalmol. 2020. PMID: 33133676 Free PMC article.
-
[Treatment of pediatric traumatic macular holes].Cesk Slov Oftalmol. 2015 Jan;71(1):30-6. Cesk Slov Oftalmol. 2015. PMID: 25959782 Czech.
-
Vitrectomy vs. Spontaneous Closure for Traumatic Macular Hole: A Systematic Review and Meta-Analysis.Front Med (Lausanne). 2021 Dec 23;8:735968. doi: 10.3389/fmed.2021.735968. eCollection 2021. Front Med (Lausanne). 2021. PMID: 35004717 Free PMC article.
-
Spontaneous closure of traumatic macular hole.Am J Ophthalmol. 2002 Feb;133(2):230-5. doi: 10.1016/s0002-9394(01)01303-4. Am J Ophthalmol. 2002. PMID: 11812427 Review.
-
Management of pediatric traumatic macular holes - case report.Case Rep Ophthalmol. 2013 Jun 6;4(2):20-7. doi: 10.1159/000350543. Print 2013 May. Case Rep Ophthalmol. 2013. PMID: 23898288 Free PMC article.
Cited by
-
Management of traumatic macular hole and retinal detachment using amniotic membrane transplantation: A case report.Am J Ophthalmol Case Rep. 2025 Feb 2;37:102267. doi: 10.1016/j.ajoc.2025.102267. eCollection 2025 Mar. Am J Ophthalmol Case Rep. 2025. PMID: 40104278 Free PMC article.
-
CORRELATIONS BETWEEN SUSPENDED HYPERREFLECTIVE MATERIAL WITH THE MACULAR MICROSTRUCTURE AND SPONTANEOUS CLOSURE OF FULL-THICKNESS MACULAR HOLES.Retina. 2024 Feb 1;44(2):237-245. doi: 10.1097/IAE.0000000000003943. Retina. 2024. PMID: 37756656 Free PMC article.
-
Traumatic macular holes: to operate, or not to operate, that is the question.Ann Transl Med. 2020 Aug;8(15):916. doi: 10.21037/atm.2020.04.50. Ann Transl Med. 2020. PMID: 32953716 Free PMC article. No abstract available.
-
Pediatric macular hole repair with amniotic membrane graft in a patient with leukemia.Am J Ophthalmol Case Rep. 2025 Jan 17;37:102259. doi: 10.1016/j.ajoc.2025.102259. eCollection 2025 Mar. Am J Ophthalmol Case Rep. 2025. PMID: 39902398 Free PMC article.
-
Characteristics and surgical outcomes of pediatric traumatic macular holes.BMC Ophthalmol. 2025 May 14;25(1):291. doi: 10.1186/s12886-025-04120-w. BMC Ophthalmol. 2025. PMID: 40369467 Free PMC article.
References
LinkOut - more resources
Full Text Sources