

Renin-angiotensin inhibitors were associated with improving outcomes of hepatocellular carcinoma with primary hypertension after hepatectomy
- PMID: 32042755
- PMCID: PMC6990038
- DOI: 10.21037/atm.2019.11.131
Renin-angiotensin inhibitors were associated with improving outcomes of hepatocellular carcinoma with primary hypertension after hepatectomy
Abstract
Background: The activation of the renin-angiotensin system (RAS) promotes tumor progression. In this study, we aimed to assess whether RAS inhibitors (RASIs) could improve the outcome of hepatocellular carcinoma (HCC) patients with primary hypertension after curative liver resection.
Methods: Data on 387 consecutive patients with primary hypertension who underwent curative liver resection for HCC were reviewed. The study population was divided into two groups based on the type of anti-hypertensive medications: the RASI group (patients using RASIs) and the non-RASI group (patients using other anti-hypertensive drugs but not RASIs). Kaplan-Meier curves, log-rank tests and cox proportional hazards regression models were used to analyze time to recurrence (TTR) and overall survival (OS).
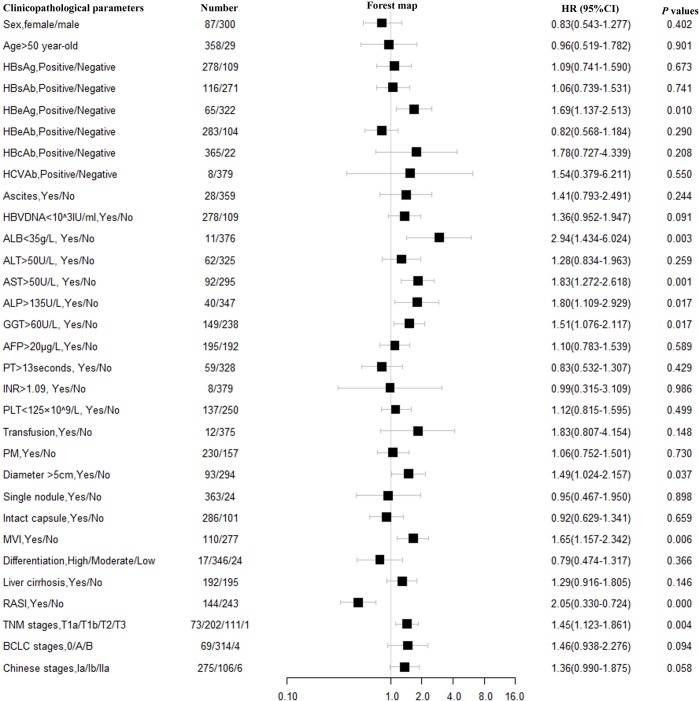
Results: There were 144 (37.2%) patients in RASI group and 243 (62.8%) in non-RASI group. The preoperative clinicopathological features were comparable between the two groups. Kaplan-Meier curves demonstrated HCC patients with RASIs had a longer TTR and OS than the patients with non-RASIs (both P<0.001). On multivariate analysis, RASIs administration was identified as an independent prognostic factor for TTR [hazard ratio (HR) =0.52, 95% confidence interval (CI), 0.38-0.70, P<0.001] and OS (HR =0.50, 95% CI, 0.34-0.74, P<0.001). Patients in the RASI group had lower rates of extrahepatic metastases than patients in the non-RASI group (2.8% vs. 7.8%, P<0.042).
Conclusions: Targeting the RAS was associated with a reduced risk of recurrence, decreased rate of extrahepatic metastases and prolonged survival of HCC patients with primary hypertension after curative liver resection.
Keywords: Hepatocellular carcinoma (HCC); hypertension; prognosis; renin-angiotensin system (RAS).
2019 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures







Comment in
-
Effects of primary hypertension treatment in the oncological outcomes of hepatocellular carcinoma.Ann Transl Med. 2020 Jul;8(14):844. doi: 10.21037/atm.2020.04.40. Ann Transl Med. 2020. PMID: 32793688 Free PMC article. No abstract available.
-
Exploring new pathways in the treatment of hepatocellular cancer.Ann Transl Med. 2020 Aug;8(16):980. doi: 10.21037/atm-20-3629. Ann Transl Med. 2020. PMID: 32953780 Free PMC article. No abstract available.
Similar articles
-
Statins and Renin Angiotensin System Inhibitors Dose-Dependently Protect Hypertensive Patients against Dialysis Risk.PLoS One. 2016 Sep 15;11(9):e0162588. doi: 10.1371/journal.pone.0162588. eCollection 2016. PLoS One. 2016. PMID: 27632175 Free PMC article.
-
Comparison of inhibitors of renin-angiotensin-aldosterone system (RAS) and combination therapy of steroids plus RAS inhibitors for patients with advanced immunoglobulin A nephropathy and impaired renal function.Clin Exp Nephrol. 2012 Apr;16(2):231-7. doi: 10.1007/s10157-011-0545-7. Epub 2011 Oct 26. Clin Exp Nephrol. 2012. PMID: 22038185
-
Renin-angiotensin system inhibitors improve the survival of cholangiocarcinoma: a propensity score-matched cohort study.BMC Cancer. 2023 Sep 5;23(1):826. doi: 10.1186/s12885-023-11152-2. BMC Cancer. 2023. PMID: 37670280 Free PMC article.
-
Association of Preoperative Renin-Angiotensin System Inhibitors With Prevention of Postoperative Atrial Fibrillation and Adverse Events: A Systematic Review and Meta-analysis.JAMA Netw Open. 2019 May 3;2(5):e194934. doi: 10.1001/jamanetworkopen.2019.4934. JAMA Netw Open. 2019. PMID: 31150082 Free PMC article.
-
Prognostic impact of renin-angiotensin system inhibitors in patients with ovarian cancer: a meta-analysis of real-world evidence.Expert Rev Anticancer Ther. 2025 Feb 6:1-9. doi: 10.1080/14737140.2025.2463486. Online ahead of print. Expert Rev Anticancer Ther. 2025. PMID: 39907527 Review.
Cited by
-
Exploring new pathways in the treatment of hepatocellular cancer.Ann Transl Med. 2020 Aug;8(16):980. doi: 10.21037/atm-20-3629. Ann Transl Med. 2020. PMID: 32953780 Free PMC article. No abstract available.
-
Effects of primary hypertension treatment in the oncological outcomes of hepatocellular carcinoma.Ann Transl Med. 2020 Jul;8(14):844. doi: 10.21037/atm.2020.04.40. Ann Transl Med. 2020. PMID: 32793688 Free PMC article. No abstract available.
-
The Importance of Metabolic Syndrome Status for the Risk of Non-Viral Hepatocellular Carcinoma: A Nationwide Population-Based Study.Front Oncol. 2022 May 4;12:863352. doi: 10.3389/fonc.2022.863352. eCollection 2022. Front Oncol. 2022. PMID: 35600376 Free PMC article.
-
System analysis based on the cuproptosis-related genes identifies LIPT1 as a novel therapy target for liver hepatocellular carcinoma.J Transl Med. 2022 Oct 4;20(1):452. doi: 10.1186/s12967-022-03630-1. J Transl Med. 2022. PMID: 36195876 Free PMC article.
-
Irbesartan inhibits metastasis by interrupting the adherence of tumor cell to endothelial cell induced by angiotensin II in hepatocellular carcinoma.Ann Transl Med. 2021 Feb;9(3):207. doi: 10.21037/atm-20-5293. Ann Transl Med. 2021. PMID: 33708834 Free PMC article.
References
-
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2018;71:e127-e248. 10.1016/j.jacc.2017.11.006 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous