

Direct observation of glucose fingerprint using in vivo Raman spectroscopy
- PMID: 32042901
- PMCID: PMC6981082
- DOI: 10.1126/sciadv.aay5206
Direct observation of glucose fingerprint using in vivo Raman spectroscopy
Abstract
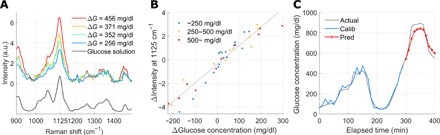
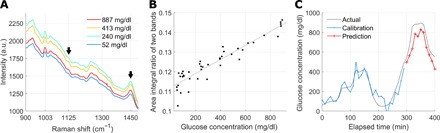
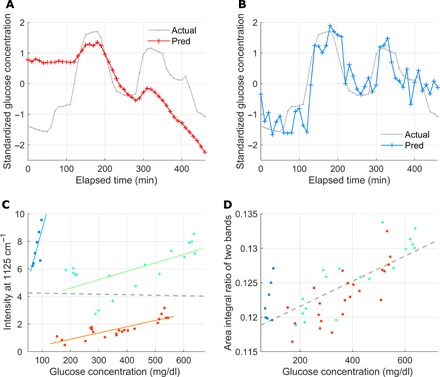
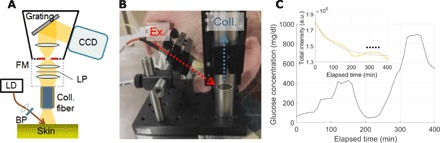
Noninvasive blood glucose monitoring has been a long-standing dream in diabetes management. The use of Raman spectroscopy, with its molecular specificity, has been investigated in this regard over the past decade. Previous studies reported on glucose sensing based on indirect evidence such as statistical correlation to the reference glucose concentration. However, these claims fail to demonstrate glucose Raman peaks, which has raised questions regarding the effectiveness of Raman spectroscopy for glucose sensing. Here, we demonstrate the first direct observation of glucose Raman peaks from in vivo skin. The signal intensities varied proportional to the reference glucose concentrations in three live swine glucose clamping experiments. Tracking spectral intensity based on linearity enabled accurate prospective prediction in within-subject and intersubject models. Our direct demonstration of glucose signal may quiet the long debate about whether glucose Raman spectra can be measured in vivo in transcutaneous glucose sensing.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works. Distributed under a Creative Commons Attribution NonCommercial License 4.0 (CC BY-NC).
Figures
References
-
- Ogurtsova K., da Rocha Fernandes J. D., Huang Y., Linnenkamp U., Guariguata L., Cho N. H., Cavan D., Shaw J. E., Makaroff L. E., IDF diabetes atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 128, 40–50 (2017). - PubMed
-
- Renard E., Monitoring glycemic control: The importance of self-monitoring of blood glucose. Am. J. Med. 118, 12S–19S (2005). - PubMed
-
- Karter A. J., Ferrara A., Darbinian J. A., Ackerson L. M., Selby J. V., Self-monitoring of blood glucose: Language and financial barriers in a managed care population with diabetes. Diabetes Care 23, 477–483 (2000). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
