

The Australasian Resuscitation In Sepsis Evaluation: Fluids or vasopressors in emergency department sepsis (ARISE FLUIDS), a multi-centre observational study describing current practice in Australia and New Zealand
- PMID: 32043315
- PMCID: PMC7496107
- DOI: 10.1111/1742-6723.13469
The Australasian Resuscitation In Sepsis Evaluation: Fluids or vasopressors in emergency department sepsis (ARISE FLUIDS), a multi-centre observational study describing current practice in Australia and New Zealand
Abstract
Objectives: To describe haemodynamic resuscitation practices in ED patients with suspected sepsis and hypotension.
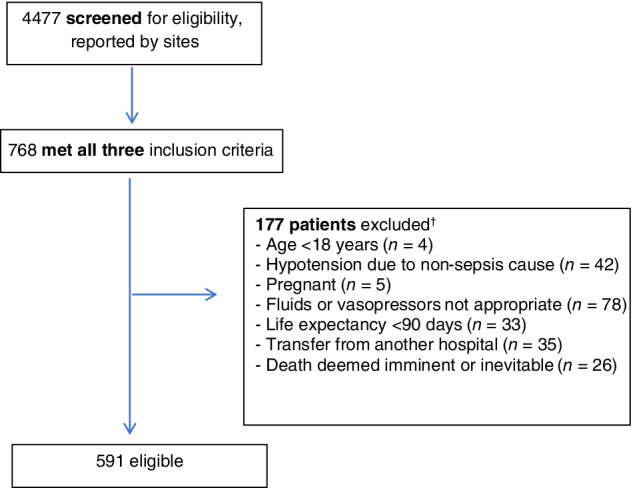
Methods: This was a prospective, multicentre, observational study conducted in 70 hospitals in Australia and New Zealand between September 2018 and January 2019. Consecutive adults presenting to the ED during a 30-day period at each site, with suspected sepsis and hypotension (systolic blood pressure <100 mmHg) despite at least 1000 mL fluid resuscitation, were eligible. Data included baseline demographics, clinical and laboratory variables and intravenous fluid volume administered, vasopressor administration at baseline and 6- and 24-h post-enrolment, time to antimicrobial administration, intensive care admission, organ support and in-hospital mortality.
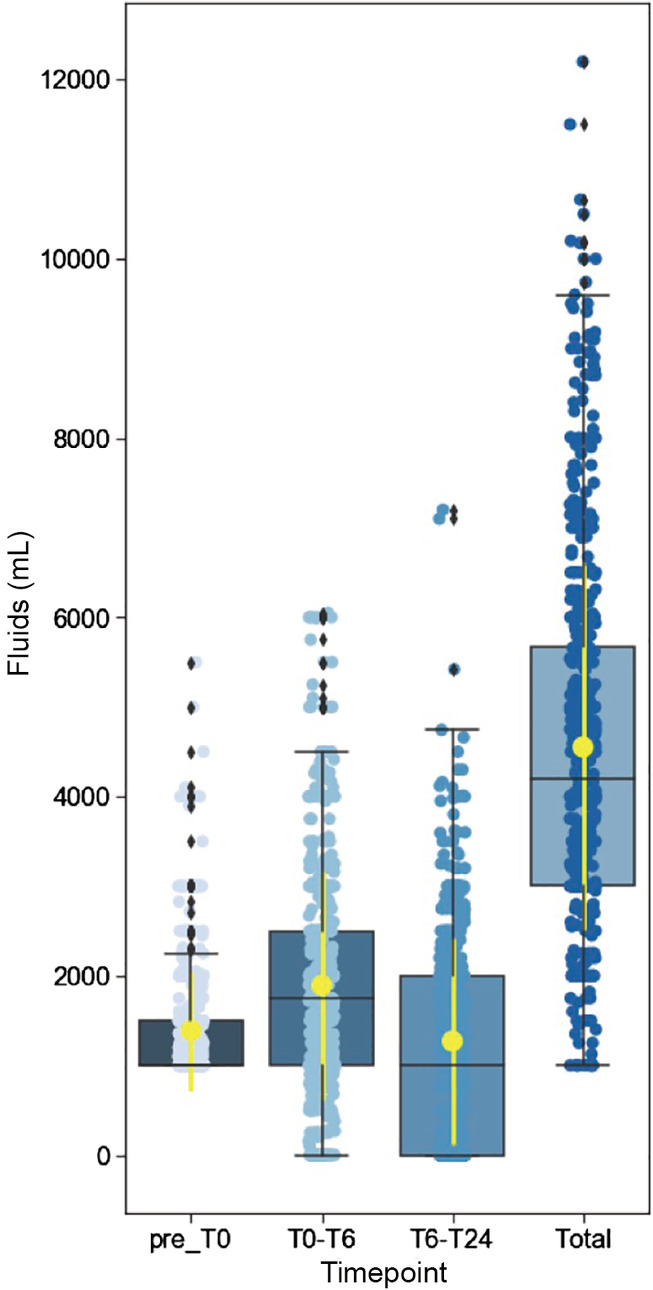
Results: A total of 4477 patients were screened and 591 were included with a mean (standard deviation) age of 62 (19) years, Acute Physiology and Chronic Health Evaluation II score 15.2 (6.6) and a median (interquartile range) systolic blood pressure of 94 mmHg (87-100). Median time to first intravenous antimicrobials was 77 min (42-148). A vasopressor infusion was commenced within 24 h in 177 (30.2%) patients, with noradrenaline the most frequently used (n = 138, 78%). A median of 2000 mL (1500-3000) of intravenous fluids was administered prior to commencing vasopressors. The total volume of fluid administered from pre-enrolment to 24 h was 4200 mL (3000-5661), with a range from 1000 to 12 200 mL. Two hundred and eighteen patients (37.1%) were admitted to an intensive care unit. Overall in-hospital mortality was 6.2% (95% confidence interval 4.4-8.5%).
Conclusion: Current resuscitation practice in patients with sepsis and hypotension varies widely and occupies the spectrum between a restricted volume/earlier vasopressor and liberal fluid/later vasopressor strategy.
Keywords: emergency department; fluid therapy; hypotension; sepsis; vasopressor.
© 2020 The Authors. Emergency Medicine Australasia published by John Wiley & Sons Australia, Ltd on behalf of Australasian College for Emergency Medicine.
Figures
Similar articles
-
The Australasian Resuscitation In Sepsis Evaluation: FLUid or vasopressors In Emergency Department Sepsis, a multicentre observational study (ARISE FLUIDS observational study): Rationale, methods and analysis plan.Emerg Med Australas. 2019 Feb;31(1):90-96. doi: 10.1111/1742-6723.13223. Epub 2019 Jan 22. Emerg Med Australas. 2019. PMID: 30669181
-
REstricted Fluid REsuscitation in Sepsis-associated Hypotension (REFRESH): study protocol for a pilot randomised controlled trial.Trials. 2017 Aug 29;18(1):399. doi: 10.1186/s13063-017-2137-7. Trials. 2017. PMID: 28851407 Free PMC article. Clinical Trial.
-
Early vs. Late Vassopressor therapy in the Management of Patients with Sepsis and Hypotension, A Multicenter Observational Study.Arch Med Res. 2021 Nov;52(8):836-842. doi: 10.1016/j.arcmed.2021.07.001. Epub 2021 Jul 16. Arch Med Res. 2021. PMID: 34275667
-
Evolving Management Practices for Early Sepsis-induced Hypoperfusion: A Narrative Review.Am J Respir Crit Care Med. 2023 May 15;207(10):1283-1299. doi: 10.1164/rccm.202209-1831CI. Am J Respir Crit Care Med. 2023. PMID: 36812500 Free PMC article. Review.
-
Emergency medicine updates: Management of sepsis and septic shock.Am J Emerg Med. 2025 Apr;90:179-191. doi: 10.1016/j.ajem.2025.01.054. Epub 2025 Jan 22. Am J Emerg Med. 2025. PMID: 39904062 Review.
Cited by
-
Effect of Out-Of-Hour Admission on Fluid Treatment of Emergency Department Patients with Suspected Infection; a Multicenter Post-Hoc Analysis.Arch Acad Emerg Med. 2023 Jan 31;11(1):e21. doi: 10.22037/aaem.v11i1.1839. eCollection 2023. Arch Acad Emerg Med. 2023. PMID: 36919142 Free PMC article.
-
Identifying septic shock subgroups to tailor fluid strategies through multi-omics integration.Nat Commun. 2024 Oct 19;15(1):9028. doi: 10.1038/s41467-024-53239-9. Nat Commun. 2024. PMID: 39424794 Free PMC article.
-
Identifying factors associated with intravenous fluid administration in patients with sepsis presenting to the emergency department: a retrospective cohort study.BMC Emerg Med. 2022 Jun 3;22(1):98. doi: 10.1186/s12873-022-00650-4. BMC Emerg Med. 2022. PMID: 35659554 Free PMC article.
-
Restrictive Fluid Administration vs. Standard of Care in Emergency Department Sepsis Patients (REFACED Sepsis)-protocol for a multicenter, randomized, clinical, proof-of-concept trial.Pilot Feasibility Stud. 2022 Mar 29;8(1):75. doi: 10.1186/s40814-022-01034-y. Pilot Feasibility Stud. 2022. PMID: 35351214 Free PMC article.
-
Australasian Resuscitation In Sepsis Evaluation: FLUid or vasopressors In emergency Department Sepsis (ARISE FLUIDS) trial: study protocol.BMJ Open. 2025 Jul 20;15(7):e101215. doi: 10.1136/bmjopen-2025-101215. BMJ Open. 2025. PMID: 40685240 Free PMC article.
References
-
- Angus DC, van de Poll T. Severe sepsis and septic shock. N. Engl. J. Med. 2013; 369: 840–51. - PubMed
-
- Rhodes A, Evans LE, Alhazzani W et al Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017; 43: 304–77. - PubMed
-
- Sirvent J‐M, Ferri C, Baro A, Murcia C, Lorencio C. Fluid balance in sepsis and septic shock as a determining factor of mortality. Am. J. Emerg. Med. 2015; 33: 186–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
