

First Description of Seronegative HTLV-1 Carriers in Argentina
- PMID: 32043459
- PMCID: PMC7124914
- DOI: 10.4269/ajtmh.19-0647
First Description of Seronegative HTLV-1 Carriers in Argentina
Abstract
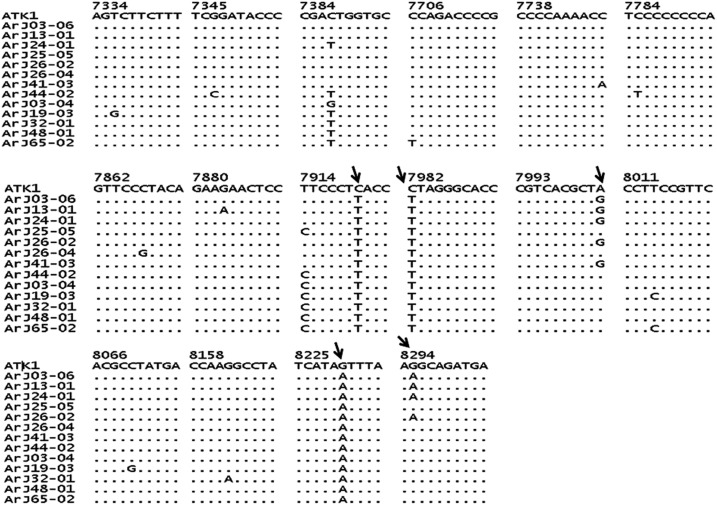
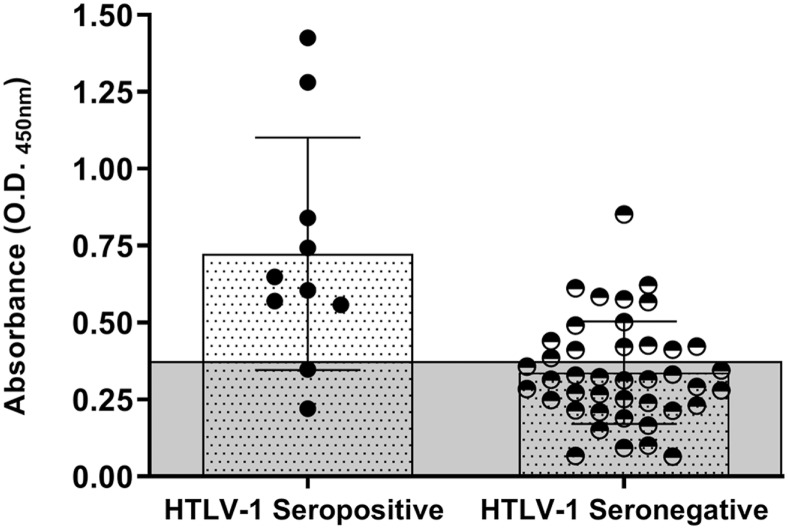
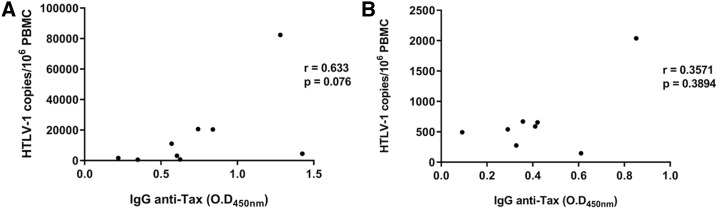
In some areas of Argentina endemic for human T-lymphotropic virus type 1 (HTLV-1), tropical spastic paraparesis is frequent in subjects who lack antibodies against the virus; however, the relevance of this seronegative status in the country has not been investigated. In neighboring countries, HTLV-1 seronegative status has been described in patients with different diseases; however, data regarding features of seronegative HTLV-1 carriers are scarce. We investigated the seronegative status in 124 relatives of 28 HTLV-1 infected subjects from an endemic area in Northwest Argentina. Blood samples and clinical/epidemiological data were collected. Human T-lymphotropic virus type 1 infection was diagnosed by serology and long terminal repeat (LTR) sequence, env and tax gene detection. IgG anti-Tax HTLV-1 antibody, tax gene sequence, and DNA proviral load were also evaluated. Seventy-five percent of the 124 relatives were negative for HTLV-1/2 antibodies; 35.5% were also negative by molecular assays and 64.5% were negative for HTLV-1 LTR and env sequences, but positive for two sequences of HTLV-1 tax gene. Also, 35.7% of these subjects had IgG anti-Tax antibodies. The seronegative HTLV-1 status was significantly associated with male gender, youth, and sensory symptoms/autonomic nervous system dysfunction. High rates of seronegative symptomatic and asymptomatic HTLV-1 carriers in Argentina are described. The evidence highlights that HTLV-1 prevalence may be underestimated worldwide. Larger cohort studies are required to assess disease outcome in these seronegative subjects. Also, the findings emphasize the limitations of ongoing screening assays for diagnosis and blood safety. Therefore, algorithms for HTLV-1 diagnosis should include not only serological but also molecular assays.
Conflict of interest statement
Disclaimer: The funders had no role in the study design, collection, analysis, and interpretation of the data, or paper writing. The first and last authors had full access to the database and take final responsibility for submitting this manuscript.
Figures
References
-
- Daenke S, Parker CE, Niewiesk S, Newsom-Davis J, Nightingale S, Bangham CR, 1994. Spastic paraparesis in a patient carrying defective human T-cell leukemia virus type I (HTLV-I) provirus sequences but lacking a humoral or cytotoxic T-cell response to HTLV-I. J Infect Dis 169: 941–943. - PubMed
-
- Ramirez E, Fernandez J, Cartier L, Villota C, Rios M, 2003. Defective human T-cell lymphotropic virus type I (HTLV-I) provirus in seronegative tropical spastic paraparesis/HTLV-I-associated myelopathy (TSP/HAM) patients. Virus Res 91: 231–239. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
