

Standardized flattening filter free volumetric modulated arc therapy plans based on anteroposterior width for total body irradiation
- PMID: 32043760
- PMCID: PMC7075390
- DOI: 10.1002/acm2.12827
Standardized flattening filter free volumetric modulated arc therapy plans based on anteroposterior width for total body irradiation
Abstract
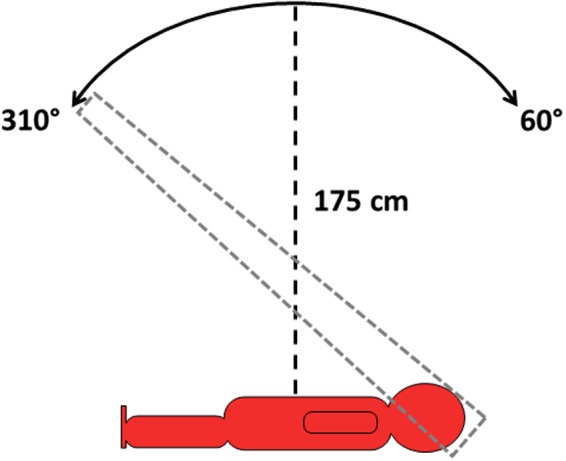
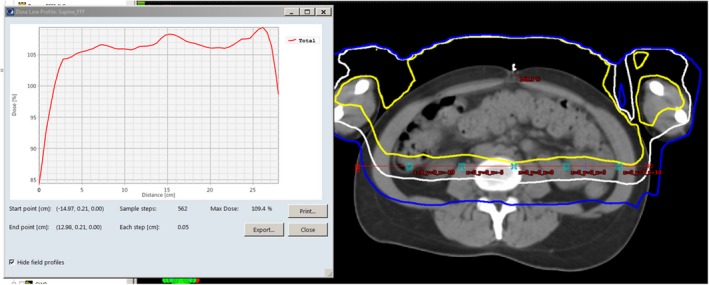
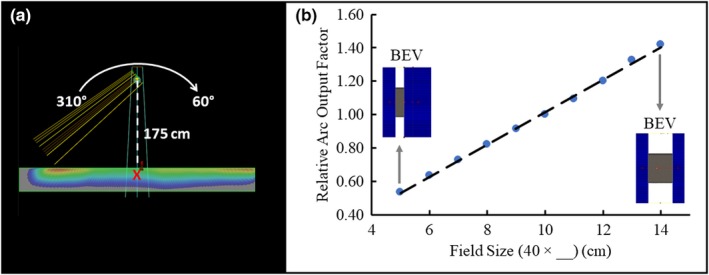
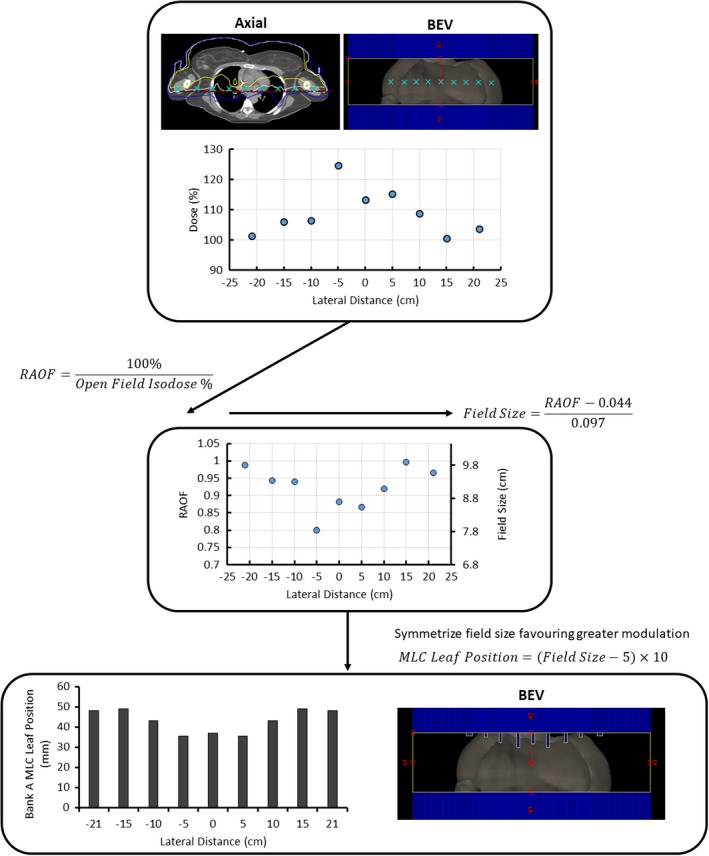
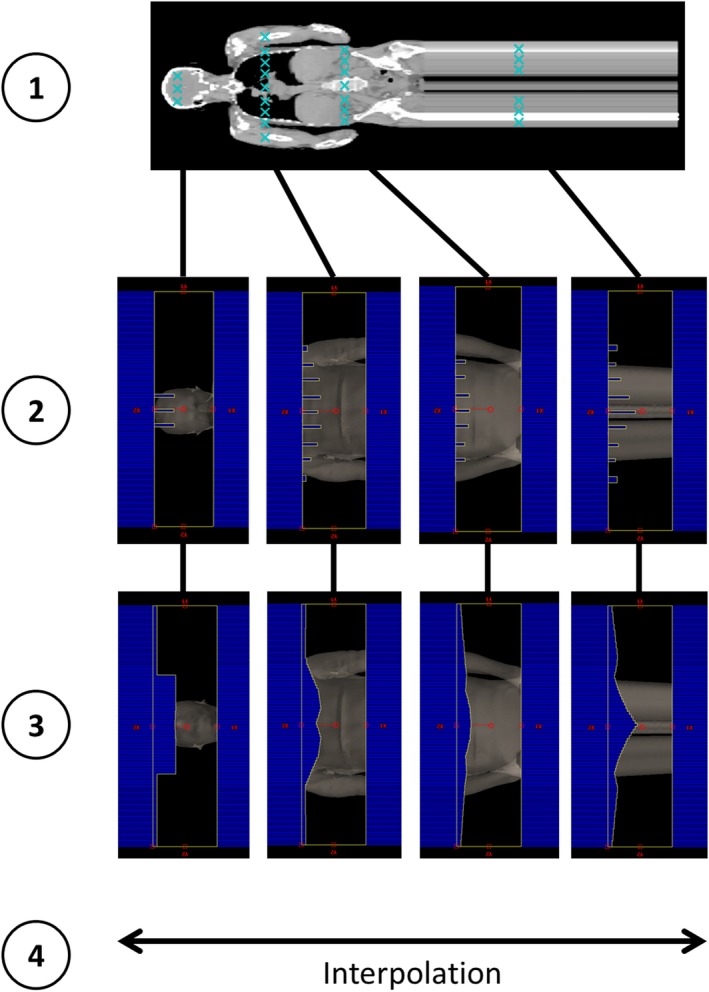
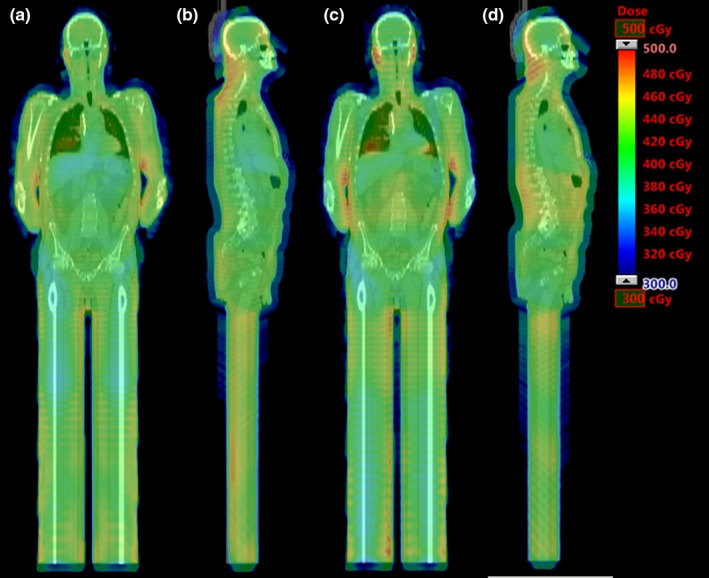
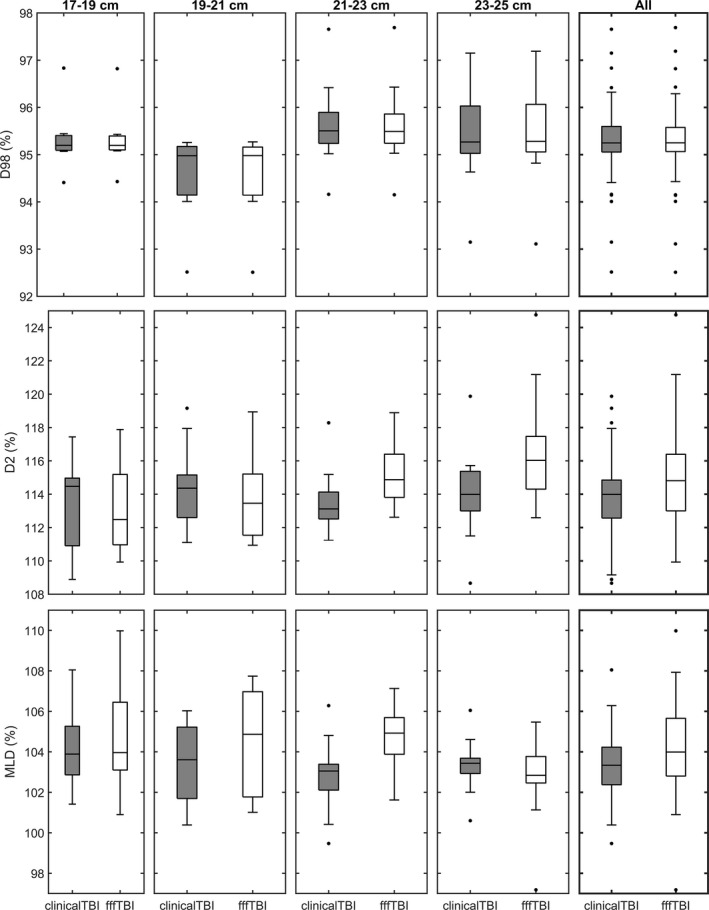
In this work, the feasibility of using flattening filter free (FFF) beams in volumetric modulated arc therapy (VMAT) total body irradiation (TBI) treatment planning to decrease protracted beam-on times for these treatments was investigated. In addition, a methodology was developed to generate standardized VMAT TBI treatment plans based on patient physical dimensions to eliminate plan optimization time. A planning study cohort of 47 TBI patients previously treated with optimized VMAT ARC 6 MV beams was retrospectively examined. These patients were sorted into six categories depending on height and anteroposterior (AP) width at the umbilicus. Using Varian Eclipse, clinical 40 cm × 10 cm open field arcs were substituted with 6 MV FFF. Mid-plane lateral dose profiles in conjunction with relative arc output factors (RAOF) yielded how far a given multileaf collimator (MLC) leaf must move in order to achieve a mid-plane 100% isodose for a specific control point. Linear interpolation gave the dynamic MLC aperture for the entire arc for each patient AP width category, which was subsequently applied through Python scripting. All FFF VMAT TBI plans were then evaluated by two radiation oncologists and deemed clinically acceptable. The FFF and clinical VMAT TBI plans had similar Body-5 mm D98% distributions, but overall the FFF plans had statistically significantly increased or broader Body-5 mm D2% and mean lung dose distributions. These differences are not considered clinically significant. Median beam-on times for the FFF and clinical VMAT TBI plans were 11.07 and 18.06 min, respectively, and planning time for the FFF VMAT TBI plans was reduced by 34.1 min. In conclusion, use of FFF beams in VMAT TBI treatment planning resulted in dose homogeneity similar to our current VMAT TBI technique. Clinical dosimetric criteria were achieved for a majority of patients while planning and calculated beam-on times were reduced, offering the possibility of improved patient experience.
Keywords: flattening filter free; total body irradiation; treatment planning; treatment technique comparison; volumetric modulated arc therapy.
© 2020 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
The authors have no relevant conflict of interest to disclose.
Figures
References
-
- Russell JA, Irish W, Balogh A, et al. The addition of 400 cGy total body irradiation to a regimen incorporating once‐daily intravenous busulfan, fludarabine, and antithymocyte globulin reduces relapse without affecting nonrelapse mortality in acute myelogenous leukemia. Biol Blood Marrow Transplant. 2010;16:509–514. - PubMed
-
- Thomas O, Mahé M‐A, Campion L, et al. Long‐term complications of total body irradiation in adults. Int J Radiat Oncol. 2001;49(1):125–131. - PubMed
-
- Van Dyk J, Galvin JM, Glasgow JP, Podgorsak EB. The Physical Aspects of Total and a Half Body Photon Irradiation. AAPM Report No 17. New York, NY: American Institute of Physics; 1986.
-
- Khan FM, Gibbons JP. Khan's the Physics of Radiation Therapy. 5th ed Philadelphia, PA: Lippincott Williams & Wilkins; 2014.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
