

Eosinophilic Fasciitis Following Checkpoint Inhibitor Therapy: Four Cases and a Review of Literature
- PMID: 32043775
- PMCID: PMC7011633
- DOI: 10.1634/theoncologist.2019-0508
Eosinophilic Fasciitis Following Checkpoint Inhibitor Therapy: Four Cases and a Review of Literature
Abstract
Background: Checkpoint inhibitor therapy is widely known to cause a number of immune-related adverse events. One rare adverse effect that is emerging is eosinophilic fasciitis, a fibrosing disorder causing inflammatory infiltration of subcutaneous fascia. It is characterized clinically by edema and subsequent induration and tightening of the skin and subcutaneous tissues. The condition is rare, yet at our institutions we have seen four cases in the past 3 years. We describe our 4 cases and review 11 other cases reported in the literature.
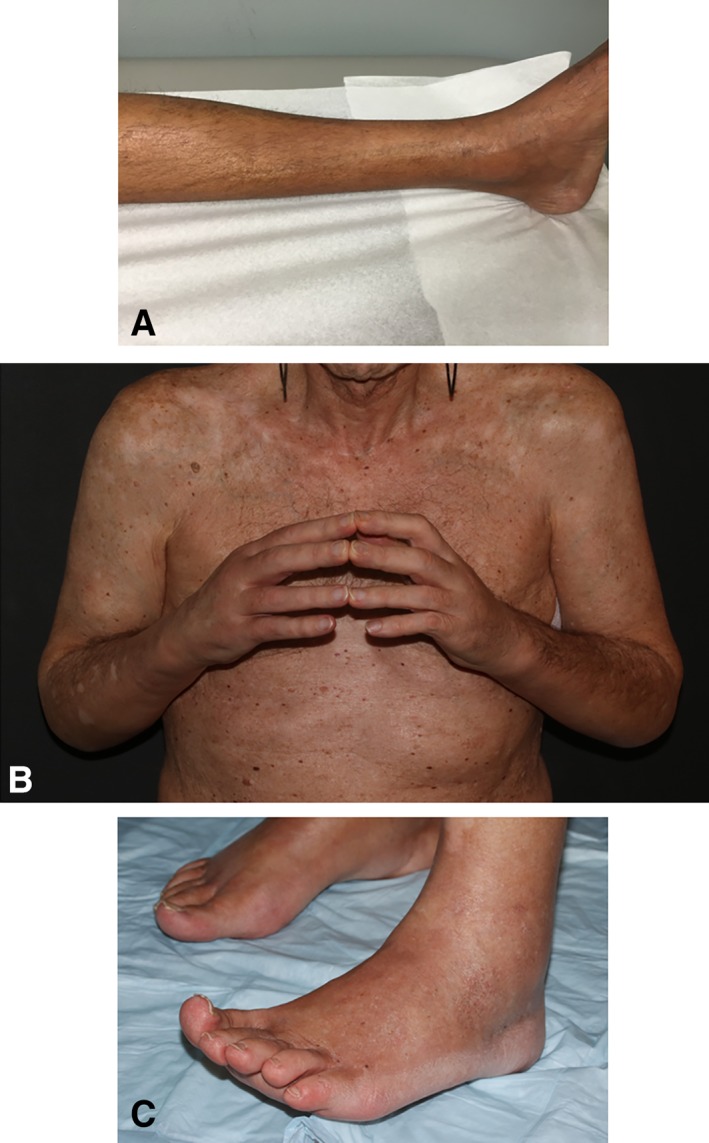
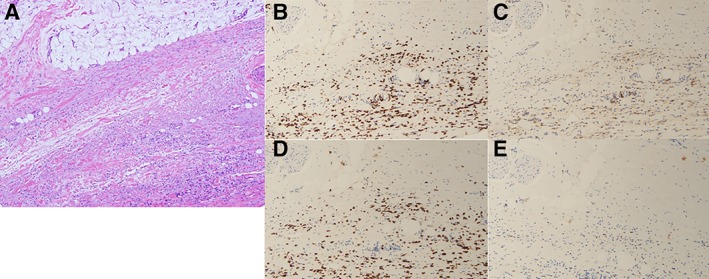
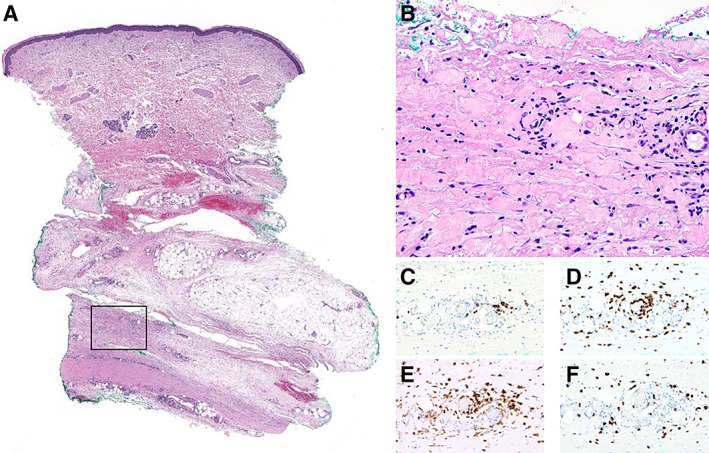
Case presentation: We present four cases of eosinophilic fasciitis following treatment with programmed cell death protein 1 or programmed cell death-ligand 1 blockade. All patients had extremity involvement with characteristic skin changes ranging from peripheral edema to induration, tightening, and joint limitation. The patients had varying degrees of peripheral eosinophilia. In two of our patients, the diagnosis was made by full-thickness skin biopsy showing lymphocytic infiltration of the subcutaneous fascia, with CD4+ T cells predominating in one case and CD8+ T cells in the other. In the other two cases, the diagnosis was made on the basis of characteristic imaging findings in the context of clinical features consistent with the diagnosis. All four patients were treated with glucocorticoids with varying degrees of success; immunotherapy had to be discontinued in all four. Patients with advanced melanoma who experienced this adverse effect had either a partial response or a complete response to therapy.
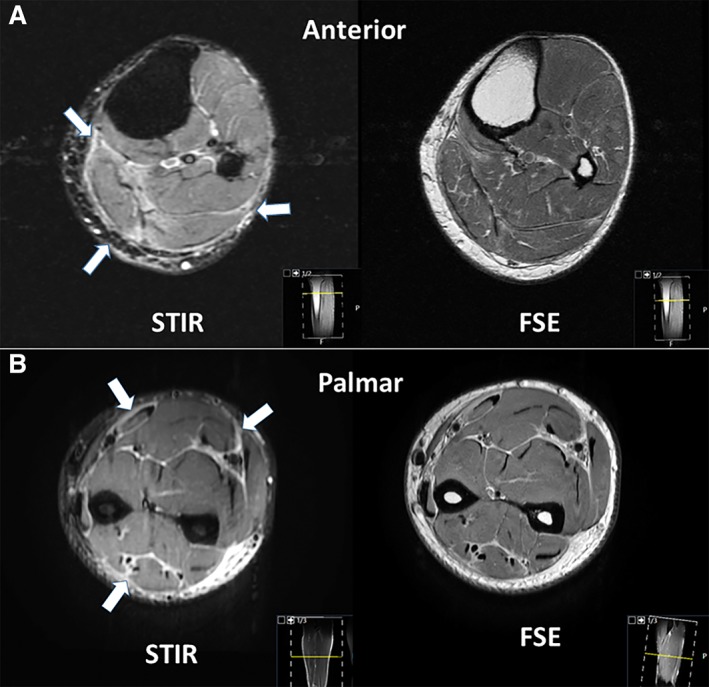
Conclusion: Eosinophilic fasciitis can occur as a result of checkpoint inhibitor therapy. Although a tissue diagnosis is the gold standard, imaging studies may facilitate the diagnosis in the presence of consistent clinical features, but a degree of suspicion is key to recognizing the condition early. Therapy requires a collaborative approach by oncology, rheumatology, and dermatology; physical therapy is an important adjunct in treatment. For advanced melanoma, it may be a good prognostic indicator.
Implications for practice: It is important for clinicians to recognize that eosinophilic fasciitis is a potential immune-related adverse event (irAE) as a consequence of immune checkpoint inhibitor therapy. The presentation is quite stereotypical; the diagnosis can be made by imaging in the absence of a full-thickness skin biopsy. Early intervention is important to limit morbidity. This irAE may be a good prognostic sign among patients with melanoma.
Keywords: Checkpoint inhibitor; Eosinophilic fasciitis; Immune-related adverse event.
© AlphaMed Press 2019.
Conflict of interest statement
Figures
References
-
- Postow MA, Sidlow R, Hellmann MD. Immune‐related adverse events associated with immune checkpoint blockade. N Engl J Med 2018;378:158–168. - PubMed
-
- Lakhanpal S, Ginsburg WW, Michet CJ et al. Eosinophilic fasciitis: Clinical spectrum and therapeutic response in 52 cases. Semin Arthritis Rheum 1988;17:221–231. - PubMed
-
- Lebeaux D, Sène D. Eosinophilic fasciitis (Shulman disease). Best Pract Res Clin Rheumatol 2012;26:449–458. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
