

Mild obstructive sleep apnea increases hypertension risk, challenging traditional severity classification
- PMID: 32043960
- PMCID: PMC7849667
- DOI: 10.5664/jcsm.8354
Mild obstructive sleep apnea increases hypertension risk, challenging traditional severity classification
Abstract
Study objectives: The association of mild obstructive sleep apnea (OSA) with important clinical outcomes remains unclear. We aimed to investigate the association between mild OSA and systemic arterial hypertension (SAH) in the European Sleep Apnea Database cohort.
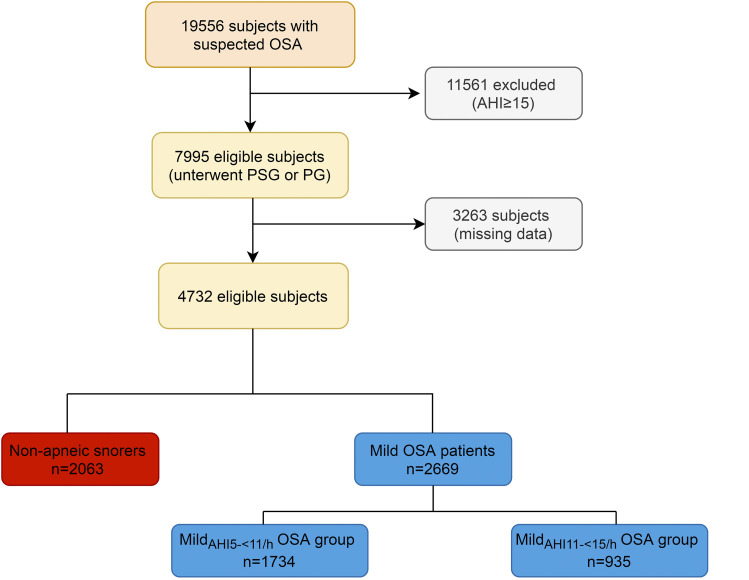
Methods: In a multicenter sample of 4,732 participants, we analyzed the risk of mild OSA (subclassified into 2 groups: mildAHI 5-<11/h (apnea-hypopnea index [AHI], 5 to <11 events/h) and mildAHI 11-<15/h (AHI, ≥11 to <15 events/h) compared with nonapneic snorers for prevalent SAH after adjustment for relevant confounding factors including sex, age, smoking, obesity, daytime sleepiness, dyslipidemia, chronic obstructive pulmonary disease, type 2 diabetes, and sleep test methodology (polygraphy or polysomnography).
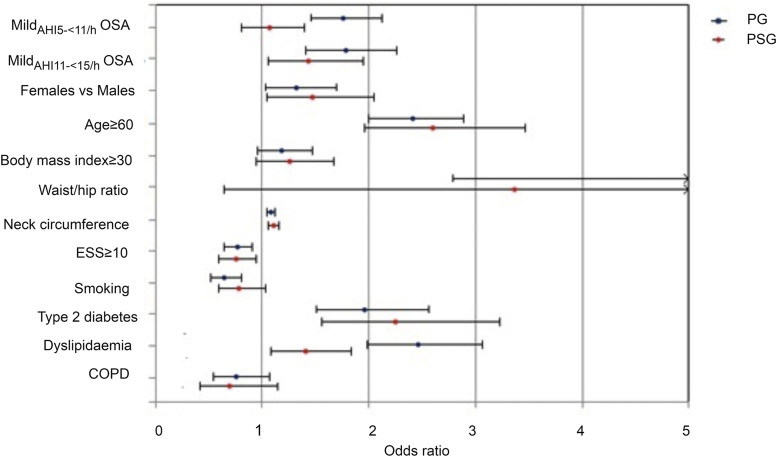
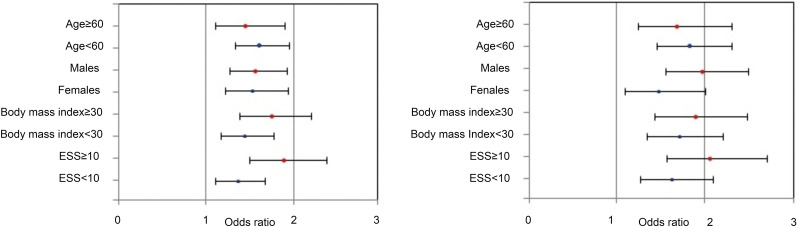
Results: SAH prevalence was higher in the mildAHI 11-<15/h OSA group compared with the mildAHI 5-<11/h group and nonapneic snorers (52% vs 45% vs 30%; P < .001). Corresponding adjusted odds ratios for SAH were 1.789 (mildAHI 11-<15/h; 95% confidence interval [CI], 1.49-2.15) and 1.558 (mildAHI 5-<11/h; 95%, CI, 1.34-1.82), respectively (P < .001). In sensitivity analysis, mildAHI 11-<15/h OSA remained a significant predictor for SAH both in the polygraphy (odds ratio, 1.779; 95% CI, 1.403-2.256; P < .001) and polysomnography groups (odds ratio, 1.424; 95% CI, 1.047-1.939; P = .025).
Conclusions: Our data suggest a dose-response relationship between mild OSA and SAH risk, starting from 5 events/h in polygraphy recordings and continuing with a further risk increase in the 11- to <150-events/h range. These findings potentially introduce a challenge to traditional thresholds of OSA severity and may help to stratify participants with OSA according to cardiovascular risk.
Keywords: European Sleep Apnea Database; mild obstructive sleep apnea; systemic arterial hypertension.
© 2020 American Academy of Sleep Medicine.
Conflict of interest statement
All authors have seen and approved the manuscript. L. Grote received grants from Bayer, Resmed, Respironics/Philips, and from the European Respiratory Society during the conduct of the study; nonfinancial support from Itamar Medical, Resmed, Philips, and Astra Zeneca, outside the submitted work; and has been issued a patent on sleep apnea therapy. J. Hedner received grants from ResMed, Respironics, and Bayer on behalf of the European Sleep Apnoea Database International Study Group; received speaker fees from ResMed, Itamar, Merck, and Jazz Pharmaceuticals outside the submitted work; and has been issued a patent on sleep apnea therapy. J. Verbraecken received grants and personal fees from ResMed, personal fees from Philips, personal fees from Sanofi, personal fees from Agfa-Gevaert, grants and personal fees from Bioprojet, grants and personal fees from Jazz Pharmaceutics, grants from AirLiquide, personal fees from Springer, grants from Westfalen Medical, grants from SomnoMed, grants from Vivisol, grants from Total Care, grants from Medidis, grants from Fisher & Paykel, grants from Wave Medical, grants from OSG, grants from Mediq Tefa, grants from NightBalance, grants from Heinen & Löwenstein, grants from AstraZen, grants from Accuramed, grants from Bekaert Deslee Academy, and grants from UCB Pharma, outside the submitted work. All other authors report no conflicts of interest.
Figures
References
-
- American Academy of Sleep Medicine . International Classification of Sleep Disorders. 3rd ed. Darien, IL: American Academy of Sleep Medicine; 2014.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
