

Concordance between current American Academy of Sleep Medicine and Centers for Medicare and Medicare scoring criteria for obstructive sleep apnea in hospitalized persons with traumatic brain injury: a VA TBI Model System study
- PMID: 32043962
- PMCID: PMC7849665
- DOI: 10.5664/jcsm.8352
Concordance between current American Academy of Sleep Medicine and Centers for Medicare and Medicare scoring criteria for obstructive sleep apnea in hospitalized persons with traumatic brain injury: a VA TBI Model System study
Abstract
Study objectives: The objective of this study was to compare obstructive sleep apnea (OSA), demographic, and traumatic brain injury (TBI) characteristics across the American Academy of Sleep Medicine (AASM) and Centers for Medicare and Medicare (CMS) scoring rules in moderate to severe TBI undergoing inpatient neurorehabilitation.
Methods: This is a secondary analysis from a prospective clinical trial of sleep apnea at 6 TBI Model System study sites (n = 248). Scoring was completed by a centralized center using both the AASM and CMS criteria for OSA. Hospitalization and injury characteristics were abstracted from the medical record, and demographics were obtained by interview by trained research assistants using TBI Model System standard procedures.
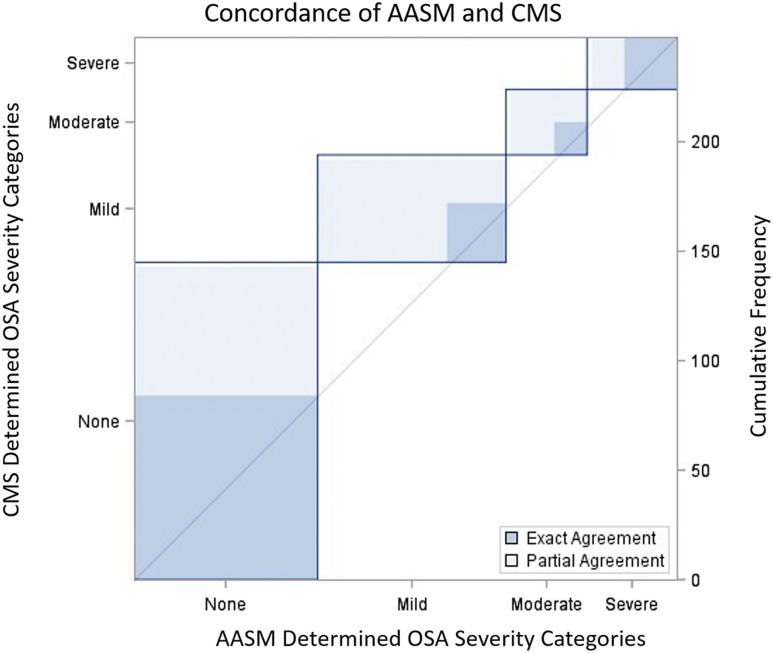
Results: OSA was prevalent using the AASM (66%) and CMS (41.5%) criteria with moderate to strong agreement (weighted κ = 0.64; 95% confidence interval = 0.58-0.70). Significant differences were observed for participants meeting AASM and CMS criteria (concordant group) compared with those meeting criteria for AASM but not CMS (discordant group). At an apnea-hypopnea index ≥ 5 events/h, the discordant group (n = 61) had lower Emergency Department Glasgow Coma Scale Scores consistent with greater injury severity (median, 5 vs 13; P = .0050), younger age (median, 38 vs 58; P < .0001), and lower body mass index (median, 22.1 vs 24.8; P = .0007) compared with the concordant group (n = 103). At an apnea-hypopnea index ≥ 15 events/h, female sex but no other differences were noted, possibly because of the smaller sample size.
Conclusions: The underestimation of sleep apnea using CMS criteria is consistent with prior literature; however, this is the first study to report the impact of the criteria in persons with moderate to severe TBI during a critical stage of neural recovery. Management of comorbidities in TBI has become an increasing focus for optimizing TBI outcomes. Given the chronic morbidity after moderate to severe TBI, the impact of CMS policy for OSA diagnosis for persons with chronic disability and young age are considerable.
Clinical trial registration: Registry: ClinicalTrials.gov; Name: Comparison of Sleep Apnea Assessment Strategies to Maximize TBI Rehabilitation Participation and Outcome; Identifier: NCT03033901.
Keywords: obstructive sleep apnea; policy; traumatic brain injuries.
© 2020 American Academy of Sleep Medicine.
Conflict of interest statement
All authors have seen and approved the manuscript. Work for this study was performed at James A. Haley Veterans’ Hospital, Tampa, Florida; Wexner Medical Center at Ohio State University, Columbus, Ohio; Harborview Medical Center, Seattle, Washington; Craig Hospital, Englewood, Colorado; Rehabilitation Hospital of Indiana, Indianapolis, Indiana; Baylor Scott and White Institute for Rehabilitation, Dallas, Texas; and Moss Rehabilitation Research Institute, Elkins Park, Pennsylvania. This study was funded by Patient-Centered Outcomes Research Institute (PCORI) Award CER-1511-33005 and was sponsored by the VHA Central Office VA TBI Model Systems Program of Research; subcontract from General Dynamics Information Technology (W91YTZ-13-C-0015 and HT0014-19-C-0004) and from the Defense and Veterans Brain Injury Center and National Institute on Disability, Independent Living, and Rehabilitation Research (NSDC Grants 90DPTB00070, 90DP0084, 90DPTB0013-01-00, 90DPTB0008, and 90DPT80004-02). The authors report no conflicts of interest. The statements presented in this publication are solely the responsibility of the author(s) and do not represent the Department of Veterans Affairs, US Government, the Patient-Centered Outcomes Research Institute (PCORI), or its Board of Governors or Methodology Committee.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
